
Tarsal Coalition
What is Tarsal Coalition?
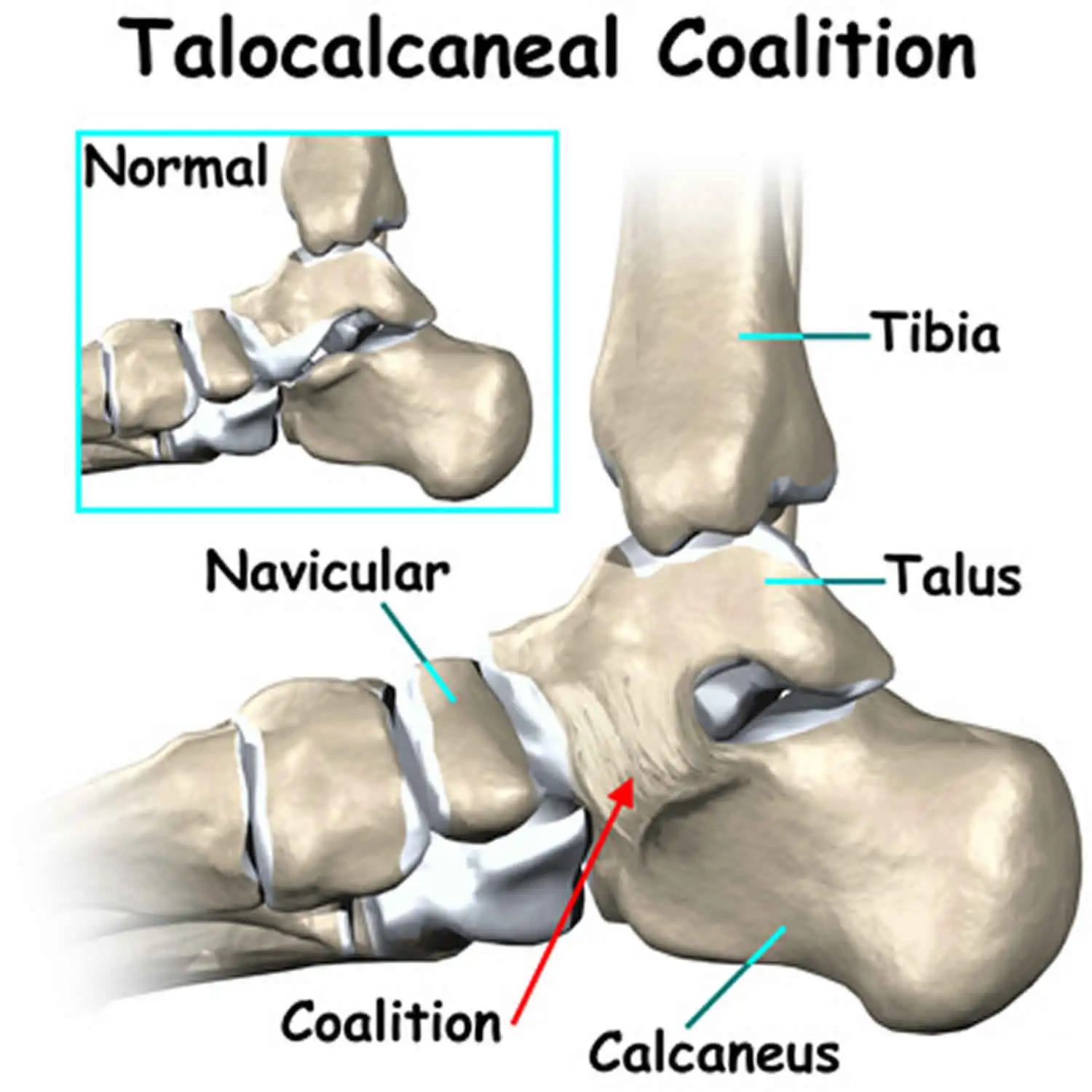
Tarsal coalition refers to a condition in which there is an abnormal connection or fusion between two or more of the tarsal bones in the foot. The tarsal bones are a group of seven bones located in the hindfoot and midfoot regions, including the talus, calcaneus, navicular, cuboid, and three cuneiform bones.
The abnormal fusion in the tarsal coalition is typically present from birth but may not become symptomatic until later in childhood or adolescence when the bones mature and become more rigid. The most common sites of the coalition are between the calcaneus and the talus (calcaneonavicular coalition) and between the talus and navicular (talocalcaneal coalition).
The exact cause of tarsal coalition is not fully understood, but it is believed to be a result of developmental abnormalities during fetal development. It may be associated with certain genetic conditions, such as multiple synostosis syndrome or fibular hemimelia, but most cases occur sporadically without any underlying genetic cause.
Fortunately, many children with tarsal coalition experience relief from their symptoms through simple treatments like orthotics and physical therapy. In cases where a child’s symptoms are severe and do not respond to these conservative measures, impacting their daily activities, surgical intervention may be recommended.
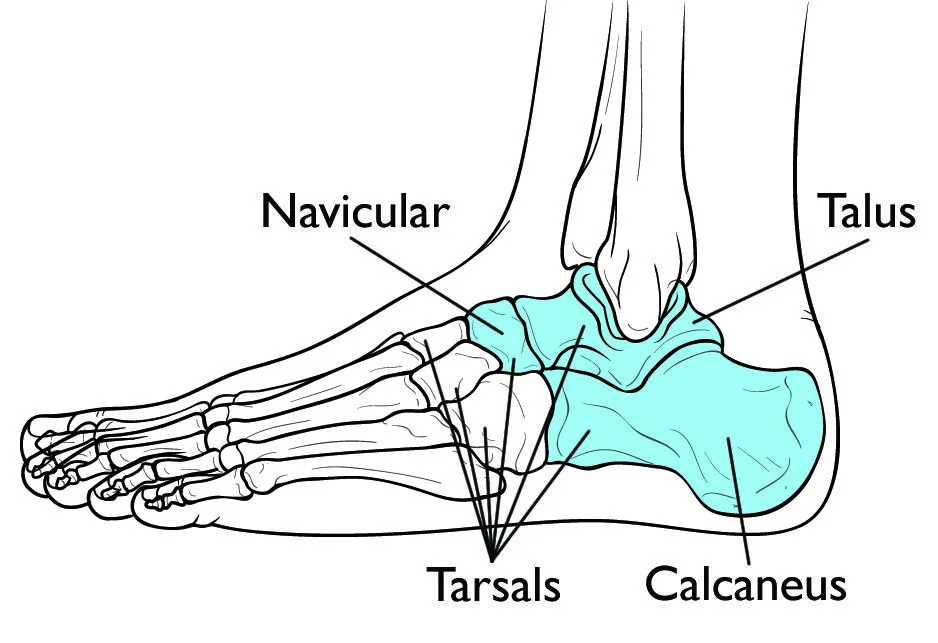
Anatomy:
The bones of the feet can be divided into three main parts: the hindfoot, midfoot, and forefoot. The hindfoot & midfoot contains 7 bones named tarsals. Among these tarsal bones, the calcaneus, talus, and navicular are the most commonly affected in cases of tarsal coalition.
The calcaneus, talus, & navicular bones are those most usually impacted in the tarsal coalition.
Description:
Tarsal coalition refers to the abnormal fusion of two bones, where a bridge of bone, cartilage, or strong fibrous tissue forms between them. These bridges, often referred to as “bars,” can either cover a small portion or a significant portion of the joint space between the bones.
The two primary sites for the tarsal coalition are between the calcaneus & navicular bones/between the talus & calcaneus bones. Regardless, other joints in the foot may furthermore be impacted.
It is estimated that approximately one out of every 100 individuals may have a tarsal coalition. About 50% of cases involve both feet. The exact prevalence of the disorder is challenging to determine because many teams do not cause noticeable symptoms.
Tarsal coalition typically develops before birth in most individuals. It is caused by a genetic mutation that affects the cells responsible for producing the tarsal bones. Although the coalition forms during fetal development, it often remains undetected until late childhood or adolescence.
During the infancy period, the foot includes a more elevated rate of gentle and developing cartilage. As a kid develops, this cartilage experiences mineralization (ossification), converting into stable, mature bone. If a coalition exists, it can furthermore experience ossification, conducting the fusion of the developing bones with a solid bridge of bone/fibrous tissue equivalent to a scar. The ossification process of the coalition typically occurs between the ages of 8 and 16, depending on the specific bones involved. Consequently, the hindfoot becomes rigid, causing pain and other associated symptoms.
The stiffness and strain caused by tarsal coalition can potentially result in arthritis over time.
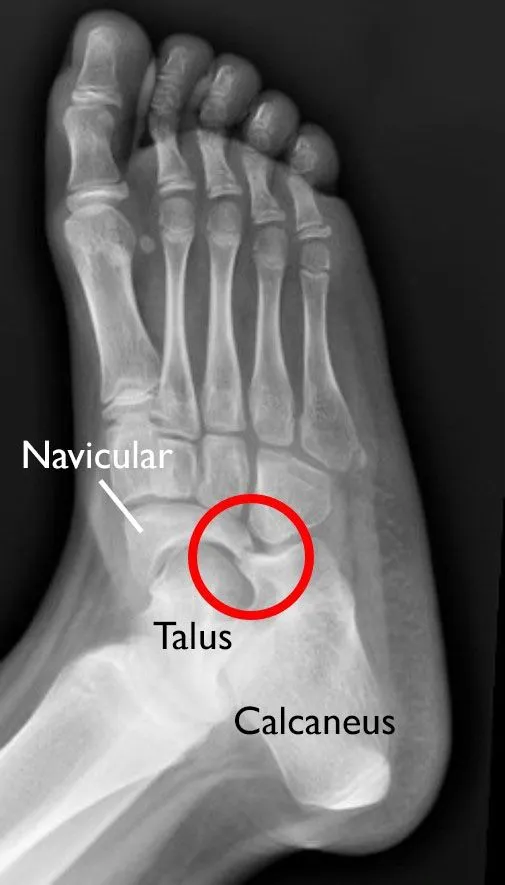
This x-ray vision of a right foot demonstrates a tarsal coalition between the navicular & the calcaneus bone.
Types of Tarsal Coalitions
- Talocalcaneal (45%)
- Calcaneonavicular (45%)
- Other: Talonavicular, Calcaneocuboid, Naviculocuneiform, Cubonavicular
The most common types of tarsal coalitions are the talocalcaneal and calcaneonavicular coalitions, accounting for approximately 45% each. However, there are other less frequent types, including talonavicular, calcaneocuboid, naviculocuneiform, and cubonavicular coalitions.
Pathological Process
In young children, the connection between the bones in a tarsal coalition is primarily cartilaginous, allowing for normal or functional motion. However, as adolescence approaches, the coalition begins to undergo ossification, potentially forming a complete or incomplete bony bridge. With the progression of ossification, the range of motion between the affected bones decreases and may eventually become entirely restricted.
When there is restricted motion in the hindfoot, it can make the foot more susceptible to twisting injuries. Normally, if a twisting force is applied to the foot, it would be dispersed among the various joints in the hind foot. However, in the presence of a tarsal coalition, this force can concentrate on a specific area, leading to an inversion sprain.
Furthermore, it has been observed that tarsal coalition is associated with a higher incidence of ankle sprains among adolescent athletes. The restricted mobility caused by the coalition may contribute to instability in the ankle joint, making it more prone to sprains during athletic activities.
Epidemiology
Tarsal coalition is a congenital condition that affects approximately 5% of the population. It tends to occur more frequently in males, with a male-to-female ratio of 4:1. Around 50% of individuals with tarsal coalition experience it bilaterally, even if symptoms are present only on one side.
One common characteristic often associated with the tarsal coalition is pes planus, which refers to a flat foot. This means that the foot arch is typically less pronounced or absent in individuals with this condition.
Symptoms of Tarsal Coalition
Many cases of tarsal coalition go undetected as they often do not manifest symptoms or lead to obvious foot deformities. Regardless, when symptoms do originate, they normally contain:
- Stiffness and pain in the feet: The pain is typically experienced below the ankle, specifically in the middle or back portion of the foot.
- Rigid and flat foot: Tarsal coalition can cause a rigid flatfoot condition, making it challenging to walk on uneven surfaces. To compensate for the limited foot motion, individuals may inadvertently roll their ankles more than usual, potentially resulting in recurrent ankle sprains.
- Increased pain or a limp during high activity levels: Engaging in activities that involve higher levels of physical exertion may intensify the pain or lead to a noticeable limp.
Diagnosis of Tarsal Coalition
Medical History and Physical Examination:

(Left) A side view of an individual with a flat foot. (Right) The foot stays flat while executing a toe raise.
Upon discussing your symptoms and overall health history, your doctor will conduct a comprehensive examination of your foot and ankle. This examination will include assessing the flexibility of your foot and observing your gait. A flat arch that doesn’t fully fix when pushing up on the toes/raising the heel while walking in a patient with tarsal coalition.
Imaging Tests:
To accurately diagnose the presence, location, and extent of the tarsal coalition(s), your doctor will request imaging tests of your foot and ankle.
X-rays: These tests provide clear images of the bones, and in many cases, tarsal coalitions can be visible on X-rays.
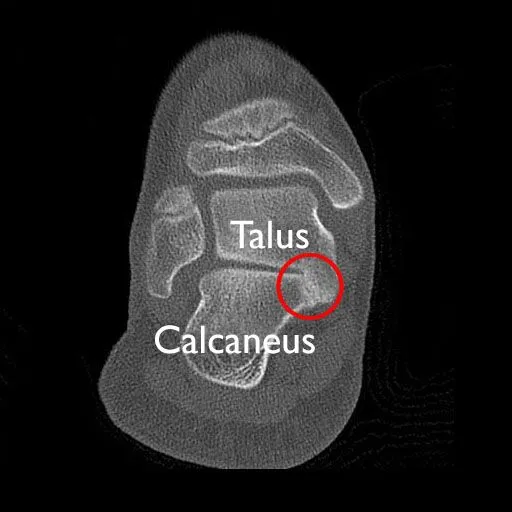
Computed Tomography (CT) scans: CT scans produce detailed images that offer a more comprehensive view of the bones. They are considered the preferred imaging method for tarsal coalitions, as they can reveal even subtle bridges or connections that might be missed on plain X-rays.
This CT picture demonstrates a cross-section outlook of the hindfoot & displays an extensive coalition merging the talus & calcaneus bones.
Magnetic Resonance Imaging (MRI) scans: MRI scans provide detailed images that encompass both bones and soft tissues. Your doctor may order this test to examine the presence of irregular bridges formed from cartilage or fibrous tissue.
Treatment of Tarsal Coalition
Tarsal coalitions generally need treatment only if they are inducing symptoms.
Nonsurgical Treatment:
- Rest: Taking a momentary pause from high-intensity movements for a period of 3-6 weeks can decrease stress on the tarsal bones & relieve pain.
- Orthotics: Arch supports, shoe inserts like heel cups and wedges, and other types of orthotics may be recommended to stabilize the foot and provide pain relief.
- Temporary immobilization: Wearing a boot or cast for a specific period can immobilize the foot, relieving stress on the tarsal bones.
- Injections: Steroid medications may be administered alongside other nonsurgical treatments to offer temporary pain relief.
- Physiotherapy management: Initial immobilization in a short-leg walking cast for 3 to 6 weeks allows irritation and inflammation to subside, enabling the child to resume athletic activities. If successful, taping the ankle and hindfoot or using an ankle brace can be encouraged for continued participation in sports. Other interventions may include nonsteroidal anti-inflammatory drugs, shoe inserts, and habit changes.
If symptoms persist despite at least 6 months of physiotherapy and conservative measures, surgical intervention may be considered.
Surgical Treatment
When non-surgical treatments fail to alleviate pain or improve function, surgery may be considered by your doctor.
The choice of surgical procedure depends on factors such as the size and location of the coalition and whether there are signs of arthritis in the affected joints.
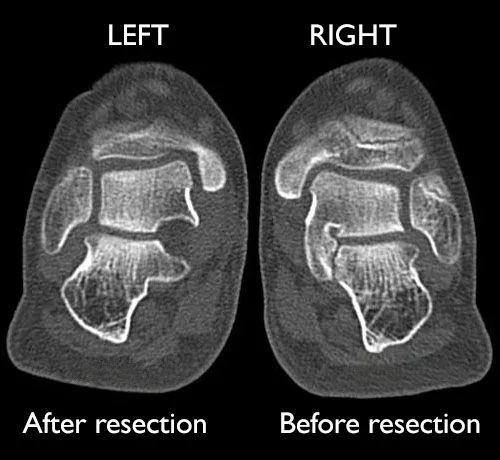
- Resection: This technique involves the subtraction of the coalition & replacing it with muscle/fatty tissue from another part of the body. It is the most common surgery for tarsal coalition and is typically recommended for patients without signs of arthritis. Resection preserves normal foot motion and effectively relieves symptoms in most cases.
These CT cross-section pictures demonstrate a patient with coalitions between the calcaneus & talus in both feet. At the duration of this scan, the alliance on the left foot had been resected, & the right foot was awaiting the process.
- Fusion: Larger & more extreme coalitions that induce marked deformity & affect arthritis may need joint fusion. The goal of fusion is to restrict the movement of painful joints and realign the bones. During fusion surgery for a tarsal coalition, large screws, pins, or screw-and-plate devices may be used to hold the bones in place.
There are different approaches for resection surgery based on the type and location of the coalition:
- Endoscopic resection may be suitable for calcaneonavicular and posterior facet talocalcaneal coalitions.
- Open resection may be indicated for anterior and middle facet involvement in talocalcaneal coalitions.
Medial excision is performed for subtalar coalitions involving the middle facet, approached through a medial hindfoot incision. Lateral excision is employed for calcaneonavicular coalitions occurring in the anterior part of the sinus tarsi, approached laterally.
Surgical excision of both calcaneonavicular & subtalar coalitions has indicated outstanding results, exact in the presence of an important talar beak.
In cases where coalition excision is unsuccessful, arthrodesis can be considered as an alternative surgical treatment for the hindfoot. However, arthrodesis eliminates pain at the expense of function, which may negatively impact athletic performance.
Postoperative Management:
Following the surgical procedure, the postoperative management will depend on the specific type of coalition excision performed:
- Postoperative Management (Medial Excision of Subtalar Coalition):
- The patient is instructed to maintain a non-weight-bearing status, with a splint worn for approximately 10 to 14 days. At the end of this duration, the skin sutures are dismissed.
- Crutches are used to assist with non-weight-bearing ambulation for 6 weeks after the surgery.
- Range of motion exercises can be initiated once the sutures are removed.
- Gradual return to activity typically occurs within a period of approximately 2 to 3 months.
- Postoperative Management (Lateral Excision of Calcaneonavicular Coalition):
- The patient is advised to remain non-weight-bearing for a period of 6 weeks.
- After the removal of sutures, usually between 10 to 14 days post-surgery, range-of-motion exercises are initiated.
- Activity is gradually increased as tolerated, following the resumption of weight-bearing.
Complications of tarsal coalition surgery
Like any surgical procedure, tarsal coalition surgery carries inherent risks. Potential complications that may arise following surgery include:
- Infection: There is a chance of acquiring an infection in the surgical area. This can generally be operated with useful wound care & in some circumstances the usage of antibiotics.
- Hematoma: Occasionally, a collection of blood (hematoma) may form at the surgical site. Drainage or additional treatment may be necessary if the hematoma causes pain or delays healing.
- Poor wound healing: In some instances, the incision site may not heal as expected, leading to delayed or poor wound healing. Close monitoring, appropriate wound care, and, in rare cases, additional interventions may be required.
- Poor bone healing: The bones involved in the surgical procedure may not heal as expected, leading to delayed union or nonunion. This can result in continued symptoms and may require additional interventions such as immobilization or revision surgery.
- Nerve injury: There is a potential risk of nerve injury during surgery, which could lead to numbness, tingling, or weakness in the foot or toes. Most nerve injuries tend to resolve with time, but in rare cases, further treatment or management may be necessary.
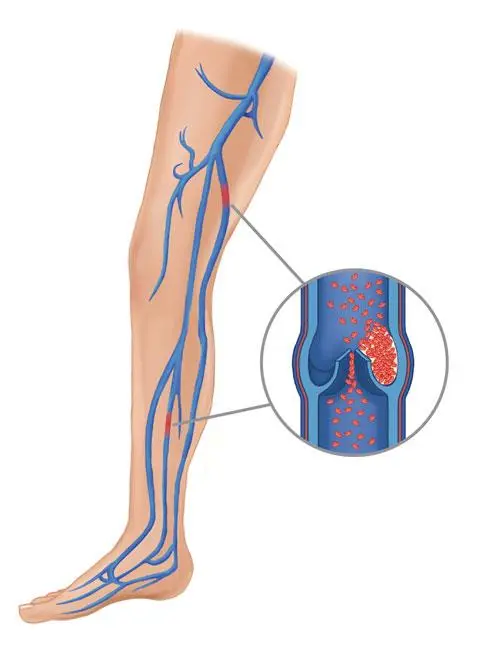
- Blood clot: Surgery can increase the risk of developing a blood clot (deep vein thrombosis). Measures such as early mobilization, compression stockings, and medications may be utilized to minimize this risk.
- Flail toes or hammertoes: In some cases, the surgical procedure may result in toe deformities such as flail toes (lack of toe control) or hammertoes (abnormal bending of the toe joints). Additional treatment options, including orthotics or corrective surgery, may be considered to address these complications.
- Stiffness or weakness in the toe: Following surgery, there is a possibility of experiencing stiffness or weakness in the toe. Physical therapy and rehabilitation may be recommended to restore normal function and mobility.
FAQs
Are there various tarsal coalition types?
There are several various kinds of tarsal coalitions. A coalition appears whenever bone cartilage/fibrous tissue develops across the joints in the foot. Most generally, this happens between the talus (ankle bone) & calcaneus (heel) bones/calcaneus & navicular bones. There are even other rare kinds of tarsal coalitions.
What if the tarsal coalition is left untreated?
In some patients, individuals may undergo adequate pain & discomfort that maintains them from the activities they enjoy. Left untreated, the tarsal coalition can induce a stiff foot after in life.
What are tips for living with a tarsal coalition?
At the first indication of a flare-up, a person should discontinue any movement that could be contributing to their symptoms. Rest is usually adequate, and if a person has endless pain, plan an appointment with a doctor. They may instruct injections/orthotics to handle pain & discomfort.
How long does it take to heal after tarsal coalition surgery?
The healing period can deviate from person to person. Generally, healing after tarsal coalition surgery takes between 6-12 months. Regardless, it may take longer relying on the person’s age, the severity of the disease, & whether or not a person has arthritis.
Can I play sports if I have a tarsal coalition?
Sports can be additionally tough for individuals with a tarsal coalition, it is conceivable to participate in athletics with the illness. If a person has been diagnosed with tarsal coalition, consult a doctor regarding any regulations.

One Comment