

Turf Toe
The simplest definition of turf toe is that it is a sprain of the main joint of the big toe. It happens when the toe is forcibly bent up into hyper-extension, such as when pushing off into a sprint and having the toe get stuck flat on the ground.
Sprains of the big toe joint became especially prevalent in American football players after artificial turf became more common on playing fields — hence the term “turf toe.” Artificial turf is a harder surface than grass and does not have much “give” when forces are placed on it.
Although often associated with football, turf toe occurs in a wide range of sports and activities.
Anatomy
The big toe is made up of two joints. The largest of the two is the metatarsophalangeal joint (MTP), where the first long bone of the foot (metatarsal) meets the first bone of the toe (phalanx). In turf toe, the MTP joint is injured.
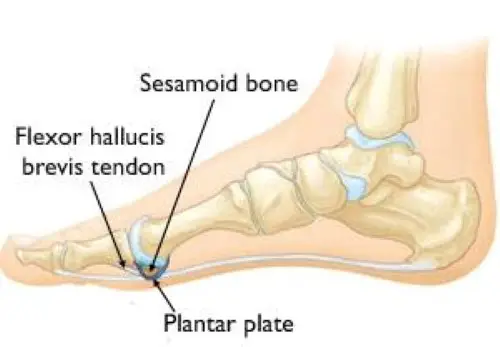
The MTP joint is surrounded by important structures that hold it in place and prevent it from dislocating. Together these structures are referred to as the “plantar complex.”
- Plantar plate. This thick, fibrous tissue under the MTP joint prevents the big toe from bending too far (dorsiflexion).
- Collateral ligaments. Located on each side of the big toe, collateral ligaments connect the phalanx bone to the metatarsal and prevent the toe from going too far side-to-side.
- Flexor hallucis brevis. This tendon runs under the first metatarsal bone and attaches to the proximal phalanx. It provides strength and stability to the big toe during push-off motions.
- Sesamoids. These two small bones are enveloped in the flexor hallucis tendon, and help it to move more easily. In addition, the sesamoids provide stability to the MTP joint by helping to bear the weight placed on the forefoot.
The slightly concave shape of the proximal phalanx with which the first metatarsal articulates creates little joint stability. The plantar capsule is thicker on the proximal phalanx and finishes in a thinner part on the metatarsal head. It supports the under-surface of the metatarsal head and resists hyper-extension of the metatarsophalangeal joint. Additionally to the plantar capsule and the collateral ligaments, the MTP joint is dynamically stabilized by the flexor hallucis brevis (FHB)(the hallucal sesamoids embedded in the FHB tendons), the adductor hallucis and the abductor hallucis tendons.
Epidemiology /Etiology
In 1976 turf toe was, for the first time, described by Bowers and Martin. They studied the soccer players at the University of West Virginia and ascertained that during one season there was an average of 5,4 turf toe injuries. Further studies showed that the injury occurred more frequently when soccer was played on artificial turf surfaces.
It is caused by an overload on the hallux MTP joint in hyper-dorsiflexion position as happens when one player falls on another players’ heel. Too strong adhesion at the surface so that the shoe sticks, while the bodyweight moves forward when the player tries to stop quickly may cause an acute turf toe. A chronical condition is mostly caused by frequent running and jumping with extremely flexible shoes. The injury results very often not due only to hyperextension but also to a degree of valgus stress.
Characteristics/Clinical Presentation
It is characterized by pain as a first symptom, localized swelling, ecchymosis, and stiffness of the joint. With an appropriate evaluation, we can divide the disease into three grades, each with its own symptoms and treatment protocols.
Grade I injury symptoms include:
Local swelling
Plantar structure’s attenuation or stretching
Minimal ecchymosis.
Grade II injury symptoms include:
Moderate swelling
Partial tear of plantar structures
Restricted motion as a result of pain.
Grade III injury symptoms include:
Indicative swelling and ecchymosis
Total disruption of the plantar structures
Weakness of the Hallux flexion
High instability of the MTP joint.
Causes
Turf toe can occur in any sport or activity when the forefoot is fixed on the ground, the heel is raised, and a force pushes the big toe into hyperextension.
These injuries most often occur among American football players on artificial grass. Artificial surfaces tend to be harder and less shock-absorbent. In addition, the athletic shoes designed for artificial surfaces are softer and more flexible, providing the athlete with more agility, but much less stability in the forefoot.
Differential Diagnosis
- Reverse turf toe
- Soccer toe
- Hallux rigidus
- Hallux limitus
- Hallux valgus
Examination
The physical examination starts with observation and palpation of the sensitivity on the hallux MTP joint, evaluating the stability and flexion strength. The palpation focuses primarily on the collateral ligaments, dorsal capsule, and the plantar sesamoid complex.
The physical examination starts with observation and palpation of the sensitivity on the hallux MTP joint, evaluating the stability and flexion strength. The palpation focuses primarily on the collateral ligaments, dorsal capsule, and the plantar sesamoid complex.
If pain is localized on the proximal sesamoids it indicates a strain of the flexor hallucis brevis musculotendinous junction, while turf toe injury is located distal to the sesamoids.
Various ranges of motion manoeuvres of the joint can also be used to identify different injuries. Comparing the active flexion strength with the contralateral side may reveal a disruption of the FHB or plantar plate.
Applying a varus and/or valgus stress to the collateral ligaments should also be performed:
- Dorsoplantar drawer test (Thompson and Hamilton) – this tests the competence of the plantar plate
- Active flexion and extension at the MTP and interphalangeal joints – this tests the extensor and flexor tendons and the plantar plate.
Medical Management
First Aid Treatment
The RICE principle is effective for most sports-related injuries when they first occur. RICE stands for Rest, Ice, Compression, and Elevation.
- Rest. Take a break from the activity that caused the injury and avoid walking or putting weight on your foot.
- Ice. Use cold packs for 20 minutes at a time, several times a day. Do not apply ice directly to the skin.
- Compression. To help prevent additional swelling, wear an elastic compression bandage.
- Elevation. To reduce swelling, recline when you rest, and put your leg up higher than your heart.
In addition, over-the-counter anti-inflammatory medications, such as ibuprofen, can help provide symptom relief.
Conservative management will always be the first line of intervention and may include Injection therapy. If conservative management is not successful then surgical intervention may be considered.
The main criteria for surgical interventions are:
- Large capsular avulsion with unstable MTP joint
- Diastasis of bipartite sesamoid
- Diastasis of sesamoid fracture
- Retraction of sesamoid
- Traumatic hallux valgus deformity
- Vertical instability (positive Lachman test result)
- Loose body in MTP joint
- Chondral injury in MTP joint
- Failed conservative treatment
Prevention
There are certain external factors that may increase the risk of turf toe injury, such as competing on artificial turf surfaces and wearing shoes with highly flexible soles. Care can be taken to ensure that your footwear is supportive and appropriate for the surface on which the sport is being played. Additionally, performing preventative flexibility and strengthening activities for the foot and ankle may improve your body’s ability to withstand the stresses placed on the body during athletic activities.
Interventions for a Grade I Injury
Once the acute phase is over, taping in slight plantar flexion, limits movement, protecting the toe from excessive range of motion, and also provides compression. Rehabilitation can begin 3 to 5 days after the injury starting with gentle, passive plantar flexion and a gradual increase in strengthening exercises. Distraction and dorsal and proximal sliding of the proximal phalanx on the first metatarsal can help to restore normal ROM and strength. The patient may participate in non-weight-bearing athletic activities such as bicycling, pool therapy and elliptical training. It’s advisable that the athlete wears stiff-soled shoes limiting the motion of the hallux.
Interventions for a Grade II Injury
A grade II turf toe injury needs at least 2 weeks before returning to activity, although the time will depend on the sport that the athlete plays. The first aim of treatment will focus on increasing the range of motion and reducing the pain, and if the athlete can tolerate it, passive joint mobilizations are indicated.
Only after the symptoms, such as pain and swelling, have been reduced can more intensive rehabilitation begin. However, care must be taken to protect the toe, either by using a turf toe plate or a Morton’s extension orthotic.
Pulsed ultrasound therapy or ionophoresis can be applied to manage inflammation and assist in the healing of the soft tissues. Active exercises can also be introduced to encourage toe extensions and flexions, such as toe crunches, curling up a towel with the toes, moving the toes in a bucket of sand, and short foot exercises. As progress is made the athlete can progress to higher-impact activities (jogging, running, cutting, and jumping).
Interventions for a Grade III Injury
The nonsurgical management of a grade III injury requires 8 weeks of recovery and immobilization in plantar flexion. Before restarting sports activity, the hallux MTP joint should return to a 50° to 60° painless, passive dorsiflexion motion. Complete rehabilitation can take up to 6 months. The most important part of the treatment for turf toe is physical therapy rehabilitation and prevention by using toe protectors/orthotics, but in certain cases, a surgical intervention may be necessary.
FAQ
How long does a turf toe take to heal?
Turf toe recovery time:
A minor case of turf toe may go away in two to three weeks if you get enough rest. The longer the toe must be immobilized and rested, the more serious the injury. Recuperation after a Grade 3 turf toe injury may need two to six months, contingent upon the need for surgery.
How do you stop turf toe?
To stop turf toe:
There are several actions you can do to avoid turf toe: When running or playing sports on hard terrain, wear shoes with a firm sole. For extra support, use athletic tape. Make use of appropriate running mechanics.
What is turf toes?
A sprain of the big toe’s primary joint is known as a “turf toe.” The metatarsophalangeal joint (MTP) is this one. Your plantar complex is made up of support components that are harmed by trauma. It occurs when you forcefully flex your big toe upward, like when you start a sprint.
Can I walk with turf toe?
For up to three weeks, you might need to use crutches or a walking boot if your turf toe is graded as Grade 3.
What happens to untreated turf toe?
Turf toe may result in bone spurs around the toe joint that may require surgical removal if treatment is not received.
Is turf toe a bad injury?
When treated promptly, turf toe injuries usually recover pretty quickly. The most frequent side effects include a variety of mild to severe, but enduring symptoms, like discomfort and stiff joints. Lack of push-off strength, stiffness, bunions, and cocking up of the big toe are possible long-term consequences.

One Comment