
Ulnar Wrist Pain
What is Ulnar Wrist Pain?
Pain on the side of your wrist opposite the thumb is known as ulnar wrist pain. Depending on the source, this discomfort might change. When you hold something or twist your wrist, it can get worse. Because it can be caused by so many various kinds of injuries, ulnar wrist discomfort can be difficult to identify.
On the outside (pinkie-finger side) of your wrist, ulnar wrist discomfort manifests. The arm bone on this side that terminates at the wrist is called the ulna. When you hold something or twist your wrist, it can get worse.
The joint connecting the hand to the forearm is referred to as the “wrist.” The wrist’s true anatomy is more complex. Eight minor bones connect the two forearm bones (radius and ulna) to the five major hand bones (metacarpals). Pain on the pinkie side of the wrist, known as ulnar wrist pain, is extremely typical. Injury to the tendons, ligaments, cartilage, or bones may cause it.
Normal anatomy
Bones and joints
The distal radius, ulna, carpal bones, and bases of the metacarpals make up the wrist. The normal range of wrist motion is made possible by the structure of the two rows of carpal bones that create smooth arcs. Gilula recognized three arcs (Gilula’s arcs) that encircle the opposing joint surface made up of the convexity of the capitate and hamate bones as well as the proximal (first arc) and distal (second arc) joint surfaces of the first carpal row(third arc).
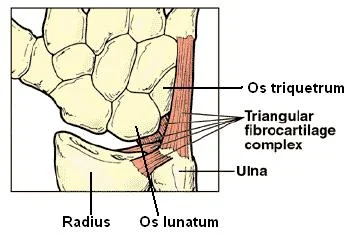
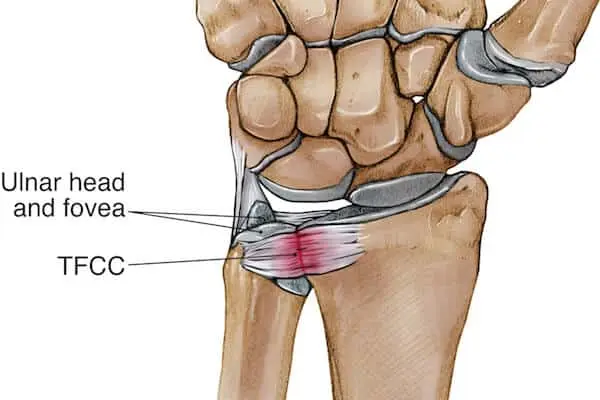
The distal ulna articulates with the triangular fibrocartilage complex (TFCC) at the ulnar aspect of the wrist. The head and the styloid process are the two eminences of the distal ulna. The head of the ulna articulates with the radius laterally and is a broad, spherical articular eminence with an oval articular surface that is distally orientated. Due to motion at the distal radioulnar joint during pronation and supination, this articulation can shift anteriorly and laterally.
The non-articular styloid process, which develops from the medial and posterior portion of the distal ulna, is where the ulnar collateral ligament originates. A little dip where the triangular fibrocartilage connects divides the styloid process from the head.
The lengths of the distal articular surfaces of the radius and ulna are referred to as ulnar variance. This variation, which is connected to a few ulnar diseases, influences the force distribution throughout the wrist.
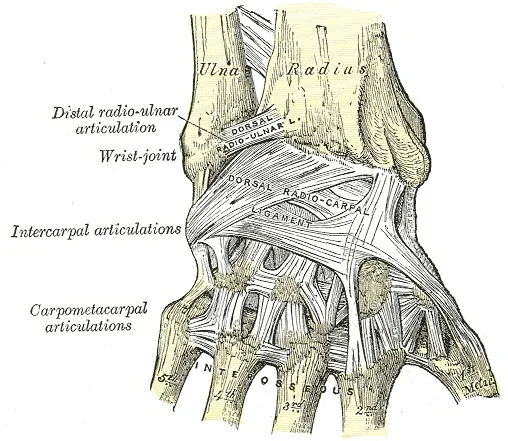
Ligaments
On the sagittal section, the lunotriquetral ligament (LTL) is U-shaped and has three distinct zones: dorsal, proximal, and volar. Ligaments can be seen in the volar and dorsal zones. The former has a crucial functional role in restricting rotation, whilst the latter transmits the triquetrum’s extension movement and is the strongest and thickest of the three zones.
The proximal zone is thin and fibrocartilaginous. Radiographically, wrists with LTL rips frequently seem normal. To show the leaking or pooling of the contrast media at the lunotriquetral interspace, arthrography might be useful. Age-related LTL proximal zone perforations, additional radiocarpal and midcarpal joint connections, and asymptomatic LTL rips on arthrography of the normal wrist have all been documented, though.
Nerve and artery
A fibro-osseous tunnel located medial to the carpal tunnel accommodates the ulnar nerve and artery as they travel through the wrist. The distal ulnar tunnel, sometimes referred to as Guyon’s canal, is a structure that runs for about 4 cm from the pisiform to the hook of the hamate. The palmar carpal ligament at the volar aspect, pisiform at the ulnar side, and the flexor retinaculum of the carpal tunnel at the radial and deep aspect defines the triangle shape of the proximal Guyon’s canal.
The volar aspect of Guyon’s canal is bordered by the palmar carpal ligament, the deep aspect by the pisohamate ligament, the ulnar aspect by the abductor digiti minimi muscle, and the radial aspect by the flexor retinaculum of the carpal tunnel. This middle portion of Guyon’s canal is between the pisiform and hook of the hamate. The ulnar nerve and artery split into deep and superficial branches in the middle of the canal.
The abductor digiti minimi muscle at the ulnar border, the palmaris brevis muscle at the volar and radial edges, and the flexor retinaculum and the hook of the hamate from the deep margin define the distal Guyon’s canal. The flexor digiti minimi brevis muscle connects to the hook of the hamate or a fibrous arch of the muscle at the distal Guyon’s canal, creating a canal that contains the deep ulnar nerve and artery as well as a superficial compartment. The superficial ulnar artery travels volar and close to the hook of the hamate just distal to Guyon’s canal. The superficial ulnar artery is more vulnerable to severe damage in this location due to its proximity to bone and lack of protecting structures above it.
Tendons
An annular ligament protects the extensor carpi ulnaris (ECU) tendon, which is located in the sixth extensor compartment at the wrist and runs in a groove at the dorsolateral portion of the ulna. At the middle of the fifth metacarpal, the ECU tendon is inserted distally. With supination and wrist extension in normal wrists, and with pronation and wrist flexion in abnormal wrists, the ECU tendon may be slightly displaced in the dorsal and volar directions, respectively.
In the distal forearm, close to Guyon’s canal, the flexor carpi ulnaris (FCU) tendon is located near the ulnar aspect of the ulnar nerve and artery. The volar limit of Guyon’s canal is formed by the FCU tendon, which inserts on the pisiform and partially combines with the palmar carpal ligament.
What are the evident indications and symptoms of an ulnar wrist condition?
Ulnar wrist discomfort is a typical symptom of a wide range of injuries and illnesses, whether it occurs at rest or during movement. The following are typical ulnar wrist discomfort symptoms and signs:
- Wrist pain on the pinky-finger side.
- You may experience a popping or clicking sound in your wrist as you move.
- Loss of hand strength when tightly grasping, accompanied by discomfort
- A reduction in wrist movement, especially when the forearm is twisted and the wrist is shifted laterally to the pinky side (ulnar deviation).
Causes of Ulnar Wrist Pain
It can be quite challenging to pinpoint the source of ulnar wrist discomfort due to the numerous components on this “pinkie” side of the wrist. Your wrist will be examined by your hand doctor to determine the source of the discomfort and how the wrist moves. X-rays might be used. Other tests, such as a CT scan or MRI, could occasionally be required.
The discomfort you feel on the outside of your wrist may be caused by a variety of different injuries and illnesses. They consist of:
- Arthritis: stiffness and inflammation in the wrist joint. This may include inflammatory arthritis, such as rheumatoid arthritis, osteoarthritis (wear and tear of the cartilage of the bones in the wrist joint), or arthritis brought on by crystal deposits from gout or pseudo-gout in the joint.
- Fractures: The fractures in which an ancient fracture involving the ulnar styloid, hook of hamate, or pisiform bones, a fractured wrist or hand, etc.
- Injury or compression to the nerves: Ulnar nerve irritation is caused by injury to or pressure on nerves in the wrist, upper arm, or neck. Neve Injury Pain, numbness, or paralysis in the wrist or hand might result from a nerve injury caused by too much pressure, straining, or even something as simple as a cut.
- Overuse: tendons and ligaments that have been harmed by repetitive movements of the hand and arm.
- Injury to the triangular fibrocartilage complex (TFCC): Tissue tears or fraying, frequently caused by a fall onto the wrist, in the tissues that link the ulna to other regions of the wrist. A developmental discrepancy in the length of the ulna relative to the nearby radius in the forearm may also cause this.
- Ulnar artery thrombosis: An ulnar artery blood clot.
- Keenbock’s condition: The lunate bone on the ulnar side of the wrist dies as a result of blood supply loss.
- Infection: from an underlying illness or earlier penetrating injury that reduced resistance to infection.
- Growths: Masses (tumors), the most frequent of which are benign ganglion cysts, are among the noncancerous tumors, masses, such as benign tumors called ganglion cysts.
- The tendons that allow the wrist to flex and extend are inflamed or irritated.
- Wrist Fractures: There’s a chance you have a wrist fracture, which is another word for a fractured wrist, regardless of how severe or mild your wrist discomfort is. Your wrist could be fractured even if you are still able to move it. Visit a hand surgeon as soon as you experience discomfort since waiting to receive treatment for a fractured wrist might be detrimental.
- Ulnar Impaction Syndrome: In people with this disease, the ulna bone might “bump into” the smaller wrist bones because it is longer than the radius bone. X-rays will probably be used by your hand surgeon to identify this issue.
- Tear TFCC: The triangle fibrocartilage complex, also known as the TFCC, is a crucial component that aids in joining the forearm to the little bones on the ulnar side of the wrist. Your wrist discomfort may be caused by a rip in it, which can happen through wear and tear or an injury.
It’s essential to see a hand surgeon as soon as possible if you have ulnar wrist discomfort. Delaying treatment might occasionally result in permanent injury and make it impossible for you to continue using your wrists for daily activities. Depending on your situation, your hand surgeon may choose from several (including non-surgical and surgical) ways to address your discomfort. To identify the source of the discomfort, your doctor may examine your wrist and perhaps order X-rays. Activity modification, splints, therapy, medication, or surgery are all possible forms of treatment.
How is ulnar wrist discomfort diagnosed?
Based on the findings of a physical examination and your medical history, doctors can identify ulnar wrist discomfort. Your doctor could inquire about things like:
- Do you have any health issues, such as diabetes, gout, or a history of infections, that may be causing your wrist pain?
- Have you ever suffered from wrist injuries before?
- Has the wrist discomfort been going on for days, weeks, or longer, or did it begin away suddenly?
- Did a certain occurrence directly cause wrist pain?
- How bad is the discomfort?
- Do your hobbies or job duties force you to use your wrists repeatedly?
Your doctor will examine your wrist and the region around it, feeling for any discomfort, swelling, redness, lumps, scars, or other deformity symptoms. In order to aid with the diagnosis, he or she will also carry out several wrist mobility tests to examine the range of motion, strength, and discomfort caused.
Additional imaging tests can be requested.
Imaging testing might consist of:
- X-rays that display the interaction between the bones of the arm and wrist can be used to spot fractures, tumors, arthritis, abnormalities, and other health issues.
- The use of computed tomography (CT) reveals minute fractures, the healing of fractures, and incorrect bone alignment. It may also detect ligament rips and examine arterial blood flow for obstructions.
- MRIs are used to look for abnormal growths and soft tissue (tendons, ligaments, blood vessels, and nerves) injuries.
- Use ultrasound to examine blood flow, evaluate aberrant growths, and locate foreign things in the wrist area as well as tendon ruptures, tendonitis, and compressed nerves.
- Before performing several of the aforementioned imaging investigations, wrist arthrography utilizes a radiopaque fluid injected into the joint to improve the image of the joint components.
When should a person make a doctor’s appointment?
You should see a doctor if you experience severe ulnar wrist discomfort that keeps you from sleeping, interferes with your ability to do your job or other everyday tasks, or is severe enough to limit your ability to move and function.
Treatment of Ulnar Wrist Pain
The diagnosis determines the course of treatment for ulnar wrist discomfort. It may involve a mix of hand treatment, steroid injections, activity adjustment, splinting or casting, and hand therapy. Surgery may be an option if non-operative therapy is ineffective in relieving symptoms.
Common methods of pain relief include:
- Using steroid injections or non-steroidal anti-inflammatory medications (NSAIDs) such as naproxen or ibuprofen or newer NSAIDs to treat pain
- Adjusting your hand’s posture ergonomically when doing repeated movements
- Exercises for the wrist’s tendons and ligaments are part of physical therapy.
- Resting the wrist with a cast or splint
- Surgery to treat arthritis, correct fractures, repair tendon or ligament tears, remove growths or other causes of nerve Compression, and replace joints as part of open or arthroscopic procedures
Physiotherapy treatment
Once the severe wrist pain has subsided, stretching exercises. As soon as stretching is almost painless, you may begin the strengthening exercises.
Stretching exercises for wrist
- Wrist flexibility
- Flexion: Bend your wrist forward slightly. Take a 5-second hold. two sets of fifteen.
- Extending: Reverse-bend your wrist slowly. Hold on for five seconds. two sets of fifteen.
- Tilt your wrist from side to side to gently shake hands. 5 seconds should be held for each direction. two sets of fifteen.
- Wrist stretch: To assist bend your wrist, press the back of the hand on the affected side with the other hand. For 15 to 30 seconds, hold. The next step is to extend the hand back by pushing the fingers backward. For 15 to 30 seconds, hold. Throughout this exercise, keep the arm on your affected side straight. Make 3 sets.
- Stand at a table with your hands facing down, your fingers flat, and your elbows straight.
- Your entire body should lean forward. For 15 seconds, maintain this posture. Do 3 Repetitions.
- Stand with your arms straight, palms up, fingers pointing in the direction of your body, and elbows straight to stretch your wrists. Turn away from the table. Keep this stance for 15 to 30 seconds. Perform 3 times.
- Pronation and supination of the forearms: Keep your injured arm’s elbow at your side while bending it 90 degrees. Hold with your palm raised for five seconds.
Strengthening exercises
- Wrist flexion: Place your palm up while holding a can or hammer handle in your hand. Raise your wrist in a bend. Return to the starting position after lowering the weight slowly. two sets of fifteen.
- Increase the weight of the can or other object you are holding gradually.
- Wrist extension: Place your palm down on the handle of a soup can or hammer.
- Raise your wrist slowly. Place the weight at the starting position and progressively reduce it.
- Two sets of fifteen. Increase the weight of the item you are holding gradually.
Summary
The majority of ulnar wrist pain diagnoses may be made with a complete medical history, physical examination, and routine radiography. More sophisticated diagnostic modalities should be taken into consideration when a diagnosis cannot be made using conventional techniques. Most of the time, when a proper diagnosis has been made, choosing an effective treatment method is simple.
FAQs
How do you fix ulnar wrist pain?
It could involve a mix of activity modification, hand rehabilitation, splinting or casting, anti-inflammatory drugs, and/or steroid injections.
Is ulnar wrist pain serious?
It’s important to see a hand surgeon as soon as possible if you have ulnar wrist discomfort. Delaying treatment might occasionally result in permanent injury and make it impossible for you to utilize your wrists for daily activities.
Does ulnar wrist pain heal itself?
You should see a doctor if you have unusual ulnar wrist discomfort that limits your wrist movement and affects your regular activities. Ulnar wrist discomfort is not self-healing.
How long does ulnar wrist pain last?
A grade 1 sprain typically heals in one to three weeks, a grade 2 sprain in three to six weeks, and a grade 3 sprain in many months.
Can typing cause ulnar wrist pain?
Gaming and Typing Movements
Hand and wrist position – Any kind of misalignment can result in symptoms, but ulnar deviation and wrist extension are by far the most detrimental. Both of these positions put a significant amount of strain on the wrist’s structures and, particularly, its nerves.





2 Comments