Anatomy of Ankle
Overview
The ankle is one of the most versatile and hardworking joints in the human body. It smoothly adjusts with each step to absorb shock, adapt to uneven terrain, and provide the stability and mobility necessary for activities from walking to jumping.
Comprised of an intricate network of bones, cartilage, ligaments, tendons, muscles, nerves, and blood vessels, the ankle structures collaborate to position the foot and translate forces from the leg to the ground. This balance of flexibility, weight-bearing capacity, and support is integral to overall health and quality of life.
Let’s explore what’s underneath that knobby round protrusion jutting out on each side of your slender ankle joint. A deeper dive into anatomy provides insight into how this body part functions, why injuries occur, and how we can keep our ankles healthy through the long mileage of life.
Anatomical Structures of Ankle
Bones
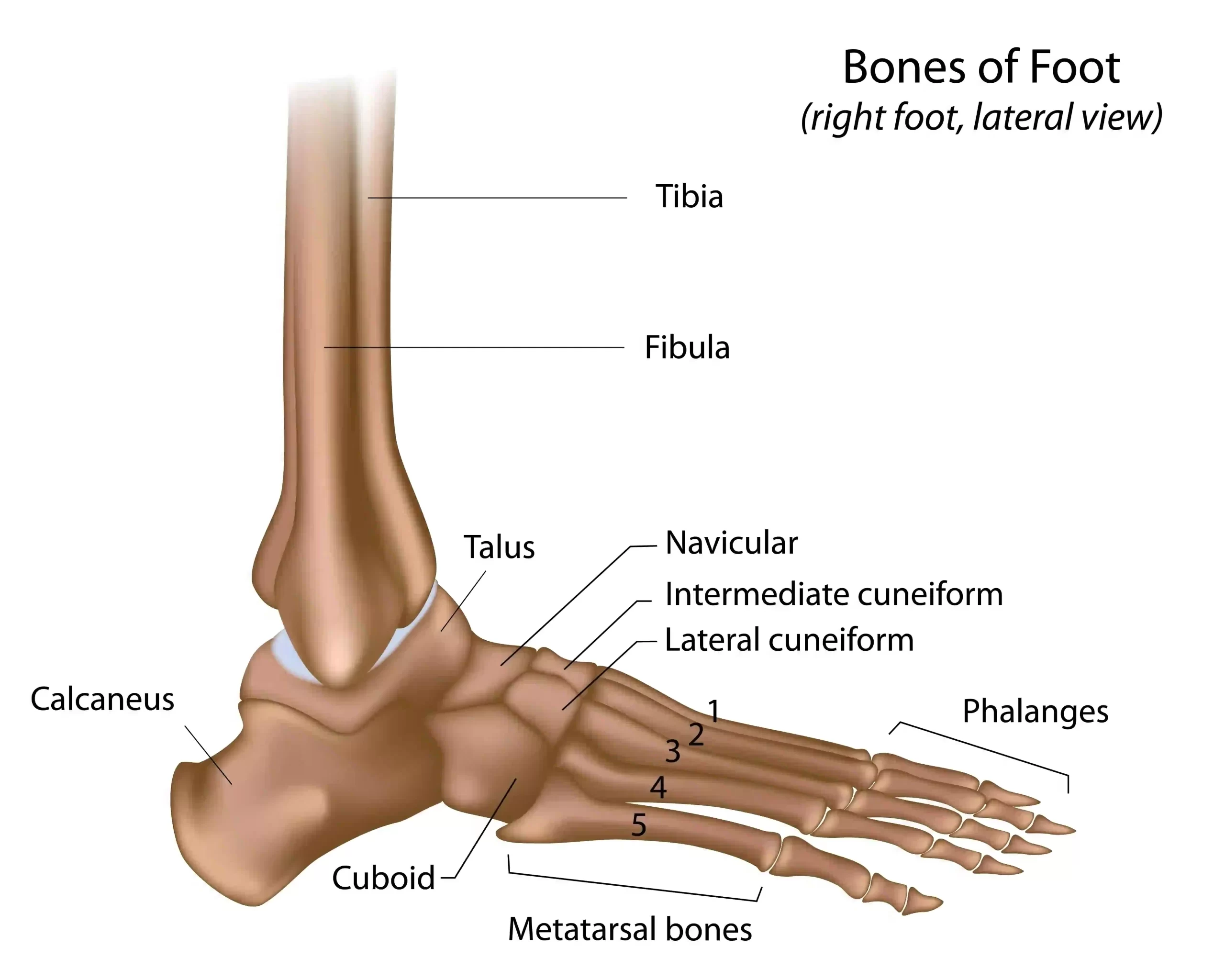
The ankle joint bones include:
• Tibia: Inner leg bone forming the medial malleolus bony ankle protrusion on the inside
• Fibula: Smaller outer leg bone forming the lateral malleolus on the outside
• Talus: Wedge-shaped foot bone that articulates between the tibia and fibula distally
These three bones intersect to compose the ankle joint, officially termed the talocrural joint. The unique shapes of complimentary articular facets allow primarily hinge-like dorsiflexion and plantarflexion while permitting slight rotation.
Tibia
The tibia is the main weight-bearing bone of the lower leg, transferring forces from the knee joint down to the ankle and foot. The distal end widens forming the medial malleolus and contributing to the ankle joint.
Specific features of tibial anatomy:
- Medial malleolus – A prominent, tooth-like bony process projecting distally that serves as an attachment point for ankle ligaments/tendons and forms the medial portion of the ankle joint
- Articular surface – Smooth concave facet on the underside of the medial malleolus that articulates with the talus to form the tibiotalar joint
- Interosseous border – Vertical ridge running the tibia’s length for interosseous membrane attachment forming a joint with adjacent fibula
- Fibular notch – Indentation on lateral distal tibia that articulates with the distal fibula
Fibula
The thinner fibula runs parallel to the tibia providing stability and forms the lateral portion of the ankle joint via the lateral malleolus.
Key fibular anatomy:
- Lateral malleolus – The distal end of the fibula expanded into a broad protrusion forming the lateral side of the ankle joint. It articulates with the talus and provides attachment points.
- Articular facet – Oblique articular surface located on the medial side of the lateral malleolus that articulates with the talus.
- Interosseous crest – Narrow vertical ridge on the medial fibula for interosseous membrane attachment site with tibia.
Talus
The talus sits at the intersection of the ankle and subtalar joints, transferring the weight of the body from the leg to the foot.
Notable talus bony landmarks:
- Head – Rounded anterior aspect with articulation facet for navicular bone
- Neck – Narrow region connecting the talus head and body
- Body – The main central region between ankle/subtalar joints bearing load
- Trochlea tali – Concave superior surface that articulates with the tibia in the ankle joint
- Lateral/medial processes – Provide stability articulating with malleoli
The squat, knobby malleoli bony protrusions on each side provide extensive stability and attachment points for supporting ligaments and tendons. They brace the talus bone like outriggers on a canoe, keeping it from tipping inside the ankle mortise joint space.
Ligaments
Ligaments are dense bands of connective tissue comprised of collagen fibers that connect bones providing joint stability. They guide the normal range of motion while limiting excessive mobility. The notable ligaments of the ankle include:
Medial (Deltoid) Ligaments:
- Tibionavicular – Extends from medial malleolus tibia to the navicular bone on medial foot. Maintains integrity of ankle mortise joint.
- Tibiocalcaneal – From medial malleolus and talus to the sustentaculum tali portion of calcaneus. Reinforces medial side of subtalar joint. Prevents overpronation.
- Anterior tibiotalar – Runs from tibia to attachment on the neck of talus anteriorly. Limits anterior displacement of talus between malleoli.
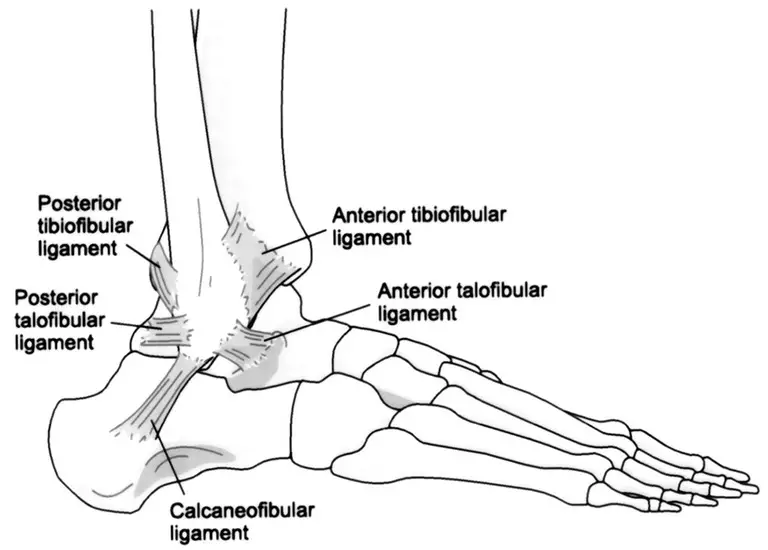
Lateral Collateral Ligaments Complex:
- Anterior talofibular ligament (ATFL) – Joins the lateral malleolus to the talus. Primary restraint against excessive inversion of the rearfoot. Most commonly injured ankle ligament.
- Calcaneofibular ligament (CFL) – Extends from lateral malleolus tip to calcaneus bone posteriorly. Stabilizes subtalar joint motion.
- Posterior talofibular (PTFL) – Lateral malleolus to back of talus. Reinforces ATFL preventing talar shift.
Syndesmosis – Assists in holding the tibia and fibula together above the ankle joint through the interosseous membrane.
These ligaments provide a supportive web restraining joint mobility within normal parameters. They guide and reinforce appropriate ankle function preventing instability or injury.
Tendons
Tendons attach muscle to bone, transducing powerful muscle contractions into joint movements. They’re comprised of dense regular connective tissue with parallel collagen fibers aligned to withstand tension. In the ankles, the key tendons are:
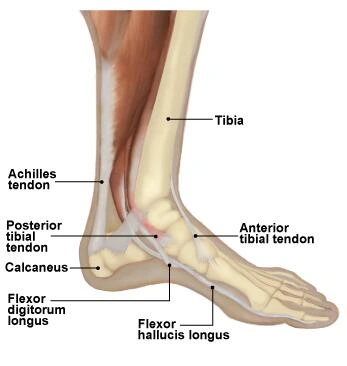
Achilles Tendon – This thick, rope-like structure anchors the gastrocnemius and soleus calf muscles to the calcaneus heel bone. When tensed, it acts like a pulley cable plantarflexing the ankle for push-off power in walking and running. This is the largest, strongest tendon in the human body capable of withstanding forces over 1000 pounds!
Anterior Tibial Tendon – Attaching shin muscles to the midfoot bones, this tendon inverts the ankle and maintains the foot’s arched structure. It bears significant tension balancing body weight across uneven terrain.
Peroneal Tendons – The peroneus longus and brevis tendons angle behind the outer ankle tethering muscles passing below the fibula malleolus. They permit ankle eversion and plantarflexion stabilizing us on one foot when pushing off while walking.
These tendons operate like biological tow ropes harnessing muscular forces to maneuver the feet–our critical contact point with the ground! Their elastic properties also store energy when stretched and then recoiling like bungee cords to boost mobility efficiency.
Muscles
While tendons link muscle to bone, muscles generate dynamic forces inducing joint movement. Key ankle movers include:
• Soleus & gastrocnemius – The muscular calf plants the foot
• Tibialis group – Pulls the foot upwards
• Fibularis/peroneal – Everts the ankle for stability
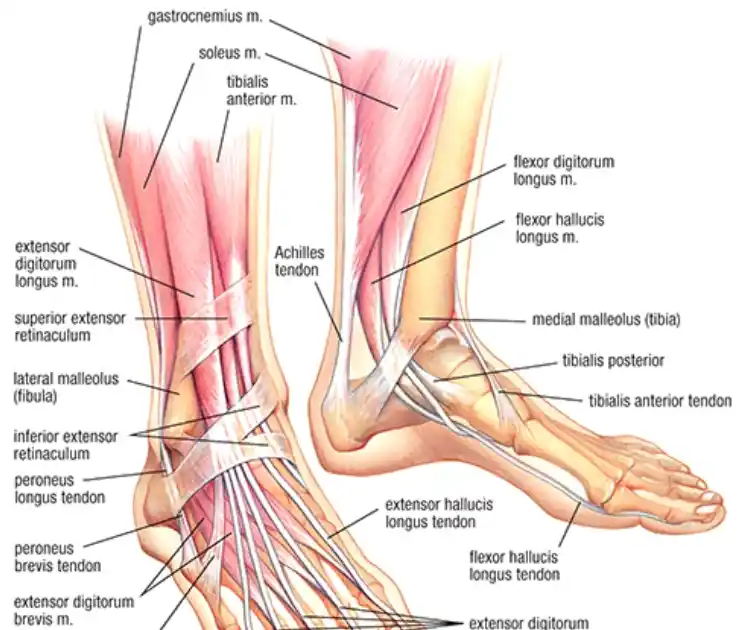
Strong muscles originating from the bones of the lower leg control ankle movements. These include:
Gastrocnemius
- Origin: Femur condyle
- Insertion: Calcaneus via Achilles tendon
- Action: Plantarflexion
- Innervation: Tibial nerve (S1, S2)
Soleus
- Origin: Tibia, fibula
- Insertion: Calcaneus via Achilles
- Action: Plantarflexion
- Innervation: Tibial nerve (S1, S2)
Tibialis Anterior
- Origin: Lateral tibia
- Insertion: Medial cuneiform, first metatarsal bone
- Action: Dorsiflexion
- Innervation: Deep fibular/peroneal nerve (L4, L5)
Tibialis Posterior
- Origin: Tibia, fibula, interosseous membrane
- Insertion: Navicular, cuneiforms, metatarsals 2-4
- Action: Plantarflexion of foot
- Innervation: Tibial nerve (L4, L5)
The coordinated strength of these muscles orchestrates overall ankle mobility. They adjust tension and length to fine-tune the positioning of the foot for adaptable support whether standing or in motion.
How Ankle Anatomy Enables Function
This symphony of anatomical elements enables the ankle’s wide range of motion, adaptability, and weight-bearing capacity. The combined efforts facilitate typical dorsiflexion upward tilt from 10-20° and plantarflexion downward motion ranging from 30-50°. This flexible hinge activity shines while walking as the ankle smoothly transitions body weight between steps.
These basic movements can be performed in isolation but more commonly intermix in functional combinations enabling abilities like running, squatting, or jumping. The ankle rocks side-to-side a touch to adjust for uneven terrain with 10-15° inversion tilting in and 5-10° eversion angles outward.
This adjustability actively stabilizes balance during transitions of body weight distribution. Meanwhile, the muscles and tendons dynamically position the foot, tightening to brace impact yet nimbly preserving mobility. The ligaments provide a last defense as sturdy bands of tissue keep the bones and joints aligned even during contortions.
During the average day, adults can tally several miles back and forth cumulative ankle motion. Now consider this versatility allows adaption from jumping sports to dancers en pointe! Our oft-ignored ankles are anatomical overachievers, quietly keeping us going through each step not just horizontally but now vertically too.
Common Ankle Injuries
Despite the intrinsic stability engineering of its anatomy, ankle trauma frequently occurs making it one of the most commonly injured body parts. Understanding the structures involved provides insight into these prevalent injuries.

Ankle Sprains
Stretching or tearing of ankle ligaments causes instability and pain termed ankle sprains. These account for the majority of all ankle injuries with a yearly incidence of 2 injuries per 1000 people. As those slender bands reinforce the joint, ligaments bear the brunt protecting the ankle bones themselves from damage.
The most commonly sprained ankle ligament is the anterior talofibular on the outer bottom front region. This ligament prevents excessive tilting of the foot downward and inward which triggers the typical injury scenario – harshly rolling the ankle.
Treatment focuses on RICE – rest, ice, compression, and elevation to allow the overstretched tissue to heal. Immobilizing with casts, walking boots or splinting helps protect the damaged ligament.
As swelling subsides, rehabilitation targets regaining flexibility and strength through physical therapy. Neuromuscular training coordinates the relationship between ankle bones, muscles, and ligaments to reestablish stability. Support taping or bracing can help during healing and return to activities.
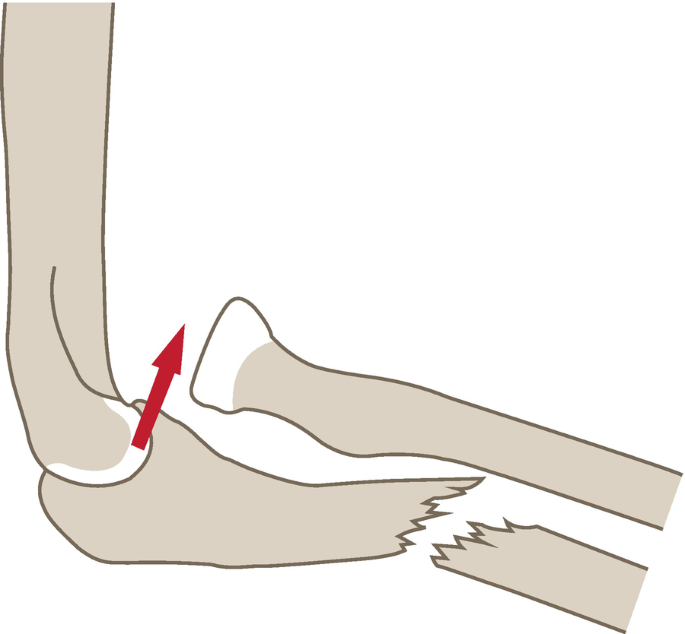
Ankle Fractures
While sprained ligaments are microtears, fractured bones constitute more traumatic, complete breaks across the tissue. Common mechanisms causing fractures include intense twisting, collisions directly impacting the ankle, or falls from heights applying immense loads upon landing.
Since the vulnerable skinny ankles bear the brunt between foot and leg, breaks often involve:
- Lower fibula bone alone or with tibia fractures
- Lateral malleolus outer ankle protrusion
- Talus ankle bone itself
The initial treatment focuses on careful realignment of any displaced broken fragment back into proper positioning to support appropriate healing. Immobilization via casts and splints aims to strictly stabilize the injury without allowing bones to settle into misaligned positions during the 4+ week bone knitting mend. In more complex fractures, surgery can involve plates and screws to reinforce stability.
As the fracture repairs over the subsequent months, physical therapy seeks to recover the range of motion and rebuild surrounding muscular strength to dynamically support the ankle.
Achilles Tendon Injuries
The various ankle tendons can endure small tears termed tendonitis due to repetitive straining or more severe ruptures if forcefully overstretched. Of these, injury involving the substantial Achilles tendon specifically disables function significantly.
As the ultimate cable tethering strong calf muscles to heel bone leverage, rupture of the Achilles severely impacts walking ability. The classic tear scenario depicts an athlete unexpectedly pushing off only for the overloaded tendon to snap and recoil up the calf in two severed ends.
Treatment starts with immobilization to allow tendon reapproximation surgically or naturally depending on the severity of the laceration. Healing aims for careful tendon reintegration to restore strength and prevent re-injury. However, regaining prior conditioning requires extensive physical therapy focused on rebuilding calf flexibility and strength.
Ankle Arthritis
While ankle sprains, fractures, and tendon injuries commonly involve younger more active people, gradual wear-and-tear arthritis plagues aging joints later in life. This chronic inflammation breaks down hyaline cartilage padding between ankle bones causing painful bone-on-bone friction.
Conservative treatment focuses on anti-inflammatory medicine, injections, bracing, shoe inserts, or using ambulatory aids to minimize discomfort associated with ankle arthritis. As joints degenerate with age, eventual surgical ankle replacement becomes an option for those with severe impairment seeking to restore mobility.
Diagnosing Ankle Injuries
Regardless of traumatic or degenerative etiology, doctors utilize imaging tests to evaluate the type and extent of ankle joint injuries.
Plain film X-rays provide initial evaluation looking at bone alignment and obvious fractures. CT scans further investigate bony trauma with 3D reconstruction for surgical planning. MRI scans best evaluate soft tissue ligaments and tendons defining tears and required repair procedures.
Understanding fundamental ankle anatomy assists physicians in recognizing injury patterns and determining proper treatment approaches.
Preventing Ankle Injuries
- Wear supportive shoes with ankle bracing and cushioning
- Strengthen ankles via stretches, resistance exercises
- Improve balance reactions through yoga, flamingo stands
- Tape or brace vulnerable ankles when active
- Warm up/cool down with stretching before sports
- Orthotics aid alignment; avoid high heels
The most protective strategy involves coupling external bracing and footwear support with internal strengthening of muscles and flexibility. This multidimensional approach furnishes the ankles with stability, shock absorption, and realignment to endure mileage. Strong, flexible ankles empower healthy longevity across the long run of life’s journeys.
Summary
The ankle is a complex hinge joint formed by three interconnected bones – the tibia, fibula, and talus. It relies on strong ligaments and the malleolar bony protrusions to provide flexibility and stabilize the joint through movements of dorsiflexion, plantarflexion, inversion, and eversion. Muscles like the gastrocnemius and soleus plantarflex the ankle while the tibialis group dorsiflexes it.
These along with delicate structures like cartilage, tendons, and blood vessels enable the ankle’s versatile range of motion necessary for shock absorption and weight distribution during functional activities from walking to jumping. Together, this anatomical collaboration between bones, muscles, ligaments, and other soft tissues powers us through each step, quietly overachieving to support the ankle’s critical role at the intersection of leg and foot.
Understanding this intricate design provides insight into how injury occurs and empowers us to proactively support healthy ankle joint function across the long mileage of life.
FAQs
What are the bones of the ankle joint?
The ankle joint involves three main bones – the tibia and fibula bones of the lower leg, and the talus bone in the foot.
How many main joints are in the ankle?
The ankle consists of two joints between those three bones, allowing a good range of motion for the foot.
What is the function of the ankle joint?
The ankle does an important job in walking and running, flexing to adapt to different ground surfaces. The main motions are up/down bending of the foot (plantar flexion and dorsiflexion), as well as some tilting inwards and outwards when combined with other foot joints.
What are the ligaments in the ankle?
To stabilize things, the ankle has three key ligament groups – the lateral ligaments on the outer ankle, the deltoid ligaments on the inner ankle, and the syndesmotic ligaments between the tibia and fibula higher up. Unfortunately with sports injuries or accidents these ligaments can become sprained or torn
How do you fix a sprained ankle?
Treating ankle sprains involves the RICE method – resting and avoiding pressure on it, applying ice packs to reduce swelling and inflammation, gentle compression bandaging, and keeping the ankle elevated higher than your heart when possible.
Is the ankle a synovial joint?
The ankle does count as a synovial joint, with a fluid-filled joint capsule allowing smooth gliding between the bones.
References:
- Sprained Ankle. (2006, December 31). WebMD. https://www.webmd.com/pain-management/ankle-sprain
- Sendić, G. (2023, October 30). Ankle joint. Kenhub. https://www.kenhub.com/en/library/anatomy/the-ankle-joint
- Professional, C. C. M. (n.d.). Ankle Joint. Cleveland Clinic. https://my.clevelandclinic.org/health/body/24909-ankle-joint
- Oiseth, S., Jones, L., & Maza Guia, E. (2024, January 10). Ankle Joint: Anatomy. Lecturio. https://www.lecturio.com/concepts/ankle-joint/
- Manganaro, D. (2023, May 23). Anatomy, Bony Pelvis, and Lower Limb: Ankle Joint. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK545158/
- Golanó, P., Dalmau-Pastor, M., Vega, J., Batista, J.P. (2014). Anatomy of the Ankle. In: d’Hooghe, P., Kerkhoffs, G. (eds) The Ankle in Football. Sports and Traumatology. Springer, Paris. https://doi.org/10.1007/978-2-8178-0523-8_1
- https://th.bing.com/th/id/R.d3db2448e99b4ca55676bbb0a3ef48a1?rik=vlL1jtyCZAjCbw&riu=http%3a%2f%2fmassagetherapyconnections.com%2fwp-content%2fuploads%2f2016%2f06%2ffoot-bones.jpg&ehk=9Jf1Q163qiJDPU2R37FA2d3JUoRJju7pB%2f%2fD6NuCwm8%3d&risl=&pid=ImgRaw&r=0
- https://cdn.shopify.com/s/files/1/1830/2553/files/tendonitis_aptoco_large.jpg?v=1535968721