

Colles Fracture
Overview
A break in the radius at the wrist is called a Colles fracture. It was given the surgeon’s name who originally described it. The break is usually seen approximately one inch (2.5 cm) below the wrist’s joining point.
One common term for a Colles’ fracture is “broken wrist.” It is sometimes referred to as a “Pouteau-Colles” fracture in France. In technical terms, it’s a fracture in your forearm’s bigger bone. The lower end of the bone fractures at its attachment to the hand’s bones on the wrist’s thumb side.
Colles fractures are common because they are the most common fractured bone in the arm. In the United States, one out of every ten shattered bones is caused by a wrist break.
The Colles fracture, which accounts for 17.5% (one-sixth) of all adult fractures that present to the emergency room, is one of the most common fractures seen in orthopedic practice. It is named after Abraham Colles, who initially reported a distal radius fracture in 1814 at the Royal College of Surgeons in Dublin. A distal radius fracture with accompanying ulnar styloid fracture, dorsal comminution, dorsal angulation, dorsal displacement, and radial shortening is referred to as a Colles fracture.
For distal fractures with dorsal angulation, the term Colles fracture is frequently used eponymously. Falling on an extended hand with the wrist in dorsiflexion frequently results in these distal radius fractures, putting strain on the volar aspect of the wrist and causing the fracture to expand dorsally.
Relevant Anatomy
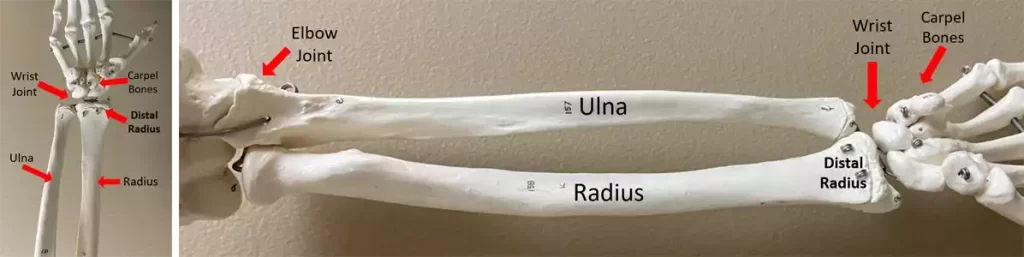
The wrist joint’s proximal side is formed by the distal radius. There, the radius articulates with the distal ulna to form a joint that permits pronation and supination, as well as with the proximal row of carpal bones to provide flexion and extension.
The triangular fibrocartilage discus (TFC), which resembles a meniscus and can be ruptured with wrist fractures, is where the distal ulna connects.
The brachioradialis inserts onto a styloid projection on the lateral side of the radius, which is also the source of the radial collateral ligament of the wrist.
The cortical thickness of the bone is smaller than the proximal and distal bone at the distal metaphysis of the radius, and the proportion of cancellous bone increases. As such, the radius’s distal metaphysis is a comparatively weak location. Fractures become more common as a result, particularly in those with lower bone mineral density.
Distal radius extra-articular fracture with low energy. maybe connected to scapholunate dissociation, ulnar styloid fracture, and TFCC (triangular fibrocartilage complex) tear.
Epidemiology
People of all ages can have distal radius fractures, but women are more likely to suffer them. There is a bimodal distribution of distal radius fractures in young athletes from high-energy injuries (e.g., motor vehicle accidents and sports-related trauma) and in elderly people from low-energy trauma. Because of the poor mineralization of the bone throughout puberty, fractures frequently occur in pediatric patients. It’s interesting to note that the age range for which these injuries are least common is 19 to 49.
It is well recognized that osteoporosis is a common cause of these fractures, which are more common in young adults and the elderly as well as in females over males. Up until the age of 75, Colles fractures are the most prevalent fractures in women in the United States and Northern Europe. Fractures of the stable Colles show little comminution.
Defined as comminuted, unstable fractures can result in avulsions of the radial or ulnar styloid, which can lead to compression neuropathies, particularly affecting the median nerve. Reflex sympathetic dystrophy and degenerative joint disease are other side effects that have been documented.
Causes of Colles Fracture
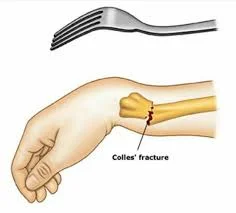
Trauma is the most frequent cause of Colles fractures. In younger patients, this typically has to do with sports-related injuries or auto accidents. The most common cause of this in the senior population is falls. The colles fracture is fractured, displaced dorsally, and frequently results in dorsal comminution when a traumatic force strikes an outstretched hand. The force is conveyed dorsally through the wrist. This process results in the well-known wrist deformity known as the “dinner fork,” which is accompanied by discomfort, edema, and a reduction in range of motion.
Many other ailments, including scapholunate, lunotriquetral ligament, distal radioulnar joint damage (DRUJ), and triangle fibrocartilage injury (TFCC), can be linked to a colons fracture. A high-energy mechanism of damage would be indicated by an accompanying radial styloid fracture.
One of the main risk factors for wrist fractures is osteoporosis. Because osteoporosis makes bones fragile, breaking them requires less power. Occasionally, the first indication of bone deterioration is a fractured wrist.
A forceful injury to the wrist results in a Colles wrist fracture. This could happen as a result of:
- Vehicle accident
- Contact Sports
- falling while biking, snowboarding, or engaging in another activity
- tripping over an extended arm (most frequent reason)
Risk Factors
The most prevalent kind of distal radial fracture, colles fractures affects all adult age groups and populations. These are very prevalent in osteoporosis sufferers. Because of this, they are most commonly observed in older ladies, especially when they fall to the ground and land on an outstretched hand.
Because osteoporosis and Colles fractures are strongly associated, a male patient who is older and has a Colles fracture should also be evaluated for osteoporosis because this increases the patient’s risk of hip fracture.
These wounds are now known as fragility fractures due to increased knowledge of osteoporosis, which suggests that an osteoporosis workup ought to be a regular component of treatment. This kind of fracture will occur more frequently as people live longer.
Aging-related osteoporosis raises the risk of these fractures in older people as well as in women, who are more likely to have osteoporosis. Particularly in women over 50, osteoporosis is a predictor of fragility fractures in the future. In women over 50, a distal radius fracture should ideally prompt a DEXA scan to evaluate the integrity of the bone.
It takes greater force to fracture the bones of younger people since their bones are stronger. Colles fractures in younger patients are typically the result of high-impact injuries or falls, such as those that occur during contact sports, skiing, horseback riding, motorcycle accidents, or falls from a height.
Types of Colles Fractures
Fractures will be categorized based on the location and mode of the bone break. This aids in figuring out the best course of action for you.
Some fracture types are as follows:
- Open fracture: Should the bone have penetrated your skin
- Comminuted fracture: if there were more than two pieces of broken bone
- Intra-articular fracture: if the wrist joint was broken by the bone
- Extra-articular fracture: if there is no harm to your joint
Symptoms of Colles Fractures
Colles fractures frequently appear clinically as a deformity resembling a dinner fork. The distal component of a distal radius fracture is posteriorly displaced, resulting in a posteriorly inclined forearm that is slightly closer to the wrist.
The patient’s hand and forearm have the curve of a dinner fork when the hand is in its typical forward arch.
- Dinner-Fork Deformity
- Fall on an outstretched hand history
- Pain in the dorsal wrist
- Wrist swelling Elevation in distal radius angulation
- Unable to grasp the object
Common Signs and Symptoms
You will have severe pain in addition to other symptoms, such as:
- Numbness
- Tenderness
- Bruising
- Swelling
- Your wrist may dangle at an unusual angle
- Reduced mobility
- wrist deformity
Frykman Classification
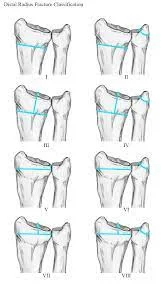
Gosta Frykman distinguished between eight distinct types of Colles fractures according to whether the fractures included the distal ends of the radius and ulna and were extra- or intra-articular.
- Type I: Transverse Metaphyseal Fracture
Include fractures of the Smith and Colles types as angulation is not a feature. - Type II: Type I + Ulnar Styloid Fracture
- Type III: Fracture Involves the Radiocarpal Joint
Comprising Chauffeur fractures as well as Barton and reverse Barton fractures. - Type IV: Type III + Ulnar Styloid Fracture
- Type V: Transverse Fracture involves Distal Radioulnar Joint
- Type VI: Type V + Ulnar Styloid Fracture
- Type VII: The radiocarpal and radioulnar joints are both involved in this comminuted fracture.
- Type VIII: Type VII + Ulnar Styloid Fracture
Diagnosis
Physical Examination
Comprehensive physical examinations of the afflicted and unaffected extremities are crucial for the diagnosis and treatment of colles fractures. During the examination, there will be wrist pain and palpable tenderness. Sometimes the fracture is displaced, and a characteristic dorsiflexion deformity, also called a “dinner fork” deformity, is observed. Visible swelling and bruises may also be present, and a complete skin examination is required to assess the possibility of an open fracture.
The injury may have reduced range of motion, but if at all possible, the clinician should evaluate it. It is critical to evaluate the neurovascular state of the extremity distal to the injury, which includes a thorough examination of the affected extremity’s pulses, sensation, and motor function. To determine whether there are any other related injuries, joints both above and below the injury must always be evaluated.
X-rays
Typically, radiographs are the primary tool used to assess, diagnose, and treat these injuries in the early stages. To evaluate these injuries, at the very least PA and lateral views should be obtained. These radiographs aid in the process of narrowing down and diagnosing the injury type among many forms of forearm fractures.
A thorough medical history that includes the mechanism of damage raises the possibility of a Colles fracture. Most commonly, a diagnosis is determined based solely on how the lateral and posteroanterior views are interpreted.
The following characteristics are present in the classic Colles fracture:
- Transverse fracture of the radius
- 2.5 centimeters, or 0.98 inches, in front of the radiocarpal joint
- Dorsal angulation and displacement, in addition to the radial tilt
- Shortening of radius
- Ulnar inclination loss
- Wrist’s radial angulation
- Crushing at the point of fracture
- More than 60% of patients had an associated ulnar styloid process fracture.
CT Scan
A CT scan is primarily recommended for surgical planning and for defining an intraarticular fracture pattern.
MRI
Though it may be used to determine the ligamentous or soft tissue extents of some injuries, such as TFCC, scapholunate, or lunotriquetral ligament injuries, an MRI is not advised as the first diagnostic measure.
Treatment of Colles Fracture
The type of Colles fracture that is present, the patient’s age and activity level, the surgeon’s choice, and the patient’s wishes regarding immobilization and return to activity will all influence the course of therapy for Colles fractures. Due to the high frequency of Colles fractures, numerous therapeutic strategies have been devised to stabilize the fractures and promote bone mending. Restoring the wrist to its previous state of functionality is the ultimate objective.
The degree of a Colles fracture determines how it should be treated. A cast by itself can be the conservative method of treating an undisplaced fracture. With the distal piece in palmar flexion and ulnar deviation, the cast is put on.
External fixation, internal fixation, percutaneous pinning, and bone replacements are among the surgical treatments available.
Closed reduction may be necessary for a fracture with modest displacement and angulation. An open reduction and internal or external fixation may be necessary for significant angulation and deformity. For the best results, use a volar forearm splint to temporarily immobilize fractures of the forearm, wrist, and hand, including Colles fractures.
The chance of operational treatment rises with an increased number of instability criteria. The optimal course of treatment will be determined after taking into account the patient’s age and physical demands, as well as the fracture pattern, degree of displacement, and stability.
Orthopedic Treatment
Orthopaedic Care and Treatment Requirements mostly on how severe the fracture is. A cast or plaster can be used as an immobilization technique for an undisplaced fracture. With the distal piece in palmar flexion and ulnar deviation, the cast is applied. Closed reduction may be necessary for a fracture with modest displacement and angulation.
There isn’t much data to support the claim that immobilizing the wrist in dorsiflexion rather than palmar flexion leads to less displacement and improved functional status. An open reduction and internal or external fixation may be necessary for significant angulation and deformity. Use a volar forearm splint for the best temporary immobilization of fractures of the hand, wrist, and forearm, including Colle’s fracture.
Several accepted criteria for instability exist:
- Dorsal tilt greater than 20°, comminuted fracture, ulnar styloid process abruption, and intraarticular
- Displacement >1mm, and loss of radial height >2mm
- A higher amount of unstable Fracture Requires operative treatment
- Treatment modalities differ in the elderly
- Regular Follow-up X-ray Examinations are Required at one, two, and six weeks to verify proper healing
- After Removal Of Cast/Fixation/Plaster Wrist Joint Stiffness Removal Physiotherapy exercises are Recommended
Physiotherapy Management
A physiotherapist will often see many patients who have discomfort, edema, reduced strength, restricted range of motion, and impaired functional abilities. To regain strength and function in the shattered wrist, rehabilitation is advised after a Colles fracture heals.
When it comes to early rehabilitation, mobilizing the wrist is the main priority. This should happen 7-8 weeks after the fracture. Early mobilization can start as soon as one week after surgery if an internal fixation device has been used to manage the fracture.
Since the wrist is frequently maintained in a pronated position, fractures that have been treated with external fixation should be handled carefully. This may put the patient at risk of developing a distal radioulnar joint contracture. Edema, cast impingement, infection, osteomyelitis, adherent scar, intrinsic or extrinsic muscle tightness, joint capsular tightness, neurovascular injury, ligament damage, and post-traumatic arthritis are other soft tissue injuries that could hinder the course of recovery.
Initial Rehabilitation
Restoring the wrist’s natural range of motion (ROM) through both passive ROM and progression to active ROM is one of the main objectives of early rehabilitation. Working within the patient’s pain-free accessible range, wrist flexion and extension are frequently the first motions stressed.
The inclusion of range-of-motion exercises aids in reducing the production of scar tissue and adhesions, which frequently follow surgery. During all stages of rehabilitation, it’s also critical to prioritize motion at the joints above and below (the elbow, fingers, and shoulder). Reducing the amount of edema and pain in the wrist and hand area is one of the main goals of early rehabilitation.
The following stage of rehabilitation for a Colles fracture still focuses on strengthening exercises and extending the wrist range of motion. Regaining range of motion (ROM) for fractures treated surgically should occur six to eight weeks after surgery.
ROM exercises that can be done include the following examples:
- Flexion and extension of wrist
- Radial and ulnar deviation
- Pronation & Supination
- Closing and opening of fist
When performing all ROM exercises with a weight in the hand or performing grip squeeze with a foam ball or towel roll, one can advance toward strengthening during the sub-acute phase. It’s crucial to strengthen not only the intrinsic and extrinsic hand muscles but also the entire forearm, gradually increasing resistance as the person gains strength.
Progressive stretching can start to expand the amount of ROM that is available during this stage. For three repetitions, each stretch should be held for 30 to 60 seconds. Ten repeats of 10 seconds can be used if the patient cannot handle a slow, prolonged stretch.
Acute Phase
Heat/Paraffin Wax
In the early stages, heat—whether from a heat pack or paraffin wax—can be quite helpful in promoting the range of motion and reducing pain. To increase venous return, it is frequently used with cold therapy.
Massage
There are two efficient massage treatments utilized in post-Colles fracture rehabilitation: massage to remove scar tissue and retrograde massage to minimize swelling. The advantage is that the patient can be taught to continue on their own when living in their own house.
Cryotherapy
Due to its capacity to assist in reducing blood flow through vasoconstriction, which limits the amount of fluid exiting from capillaries to the interstitial fluid, cryotherapy is an efficient method for controlling edema during the acute phase following trauma and during rehabilitation. Compression and elevation can also be used in conjunction with cryotherapy to treat edema. Applying cryotherapy to the affected area for ten to fifteen minutes can help manage pain for up to two hours after the treatment.
Cryotherapy should not be used on patients who are very young or very old, over a superficial branch of the nerve, over an open wound, or who have weak sensibility or mentation.
Acute febrile sickness, vasospasm (such as Raynaud’s disease), cryoglobinemia, and cold urticaria are among the conditions that preclude the use of cryotherapy.
Electrical Stimulation
Transcutaneous electrical nerve stimulation (TENS) is a pain management technique that can be used as an adjuvant at any stage of rehabilitation. However, patients who are increasing their wrist activity may find TENS to be very helpful. It is possible to interrupt the pain cycle with conventional (high-rate) TENS by using a lengthy treatment session that lasts up to twenty-four hours a day.
Another electrical stimulation method that effectively reduces pain by acting on the motor or nociceptive A-delta neurons is low-rate TENS. It has been observed that low-rate TENS can effectively manage pain for up to four or five hours after therapy.
The body of research on this subject is still inconclusive, and the findings of one study may support or contradict those of another. However, there is proof of the advantageous effects of electrical stimulation, particularly when used in conjunction with physiotherapy activities.
Exercise
Exercise is essential for strengthening the hand, wrist, elbow, and shoulder as well as for restoring range of motion. A wrist immobility significantly reduces both power and range of motion. Simple hand exercises like walking up the wall can improve range of motion (ROM), while wrist strengthening activities like writing, drawing, and shredding paper are excellent for hand strength and dexterity.
For ADLs to operate better and regain independence, the ability to utilize opposition and pinching is essential. After a Colles fracture, even seemingly easy tasks like buttoning a blouse might become challenging.
Differential Diagnosis
Other forms of distal radius fractures and other forearm fractures that can be distinguished by radiographic imaging are included in the differential diagnosis for Colles fractures.
- Smith fracture: The Smith fracture, often known as a “reverse Colles,” is typically caused by a FOOSH in supination rather than pronation and entails volar (as opposed to dorsal) angulation of the distal radial fragment.
- Barton fracture: Another kind of distal radius fracture that affects the dorsal rim of the distal radius and causes an oblique intra-articular fracture is called a Barton fracture.
- Hutchinson or Chauffer fracture: Chauffer or Hutchinson fractures, sometimes referred to as intra-articular radial styloid fractures, typically manifest as oblique or transverse fractures to the radial styloid resulting from direct trauma.
- Galeazzi fracture: Fractures to the medial or distal radius that cause the distal radioulnar joint to dislocate.
- Monteggia fracture: Fracture of the ulnar shaft accompanied by radial head dislocation.
- Essex Lopresti lesion: This is an uncommon instance of a combination of Monteggia and Galeazzi fractures involving an elbow radial head fracture, wrist DRUJ disruption, and forearm interosseous membrane rupture.
Complications
Typically, the most prevalent side effect is wrist stiffness. After taking off your cast after a month or two, it ought to become better. Additional issues consist of:
- An excruciating illness known as compartment syndrome is the result of excessive pressure inside and around your muscles.
- Malunion is the inability of the bones to unite.
- When you have median nerve palsy, your hand muscles become paralyzed, making it impossible for you to flex your thumb or touch your fingers.
- The wrist nerves are compressed when you have carpal tunnel syndrome. The wrist and hand pain, numbness, and weakness are the symptoms.
- Burning pain in the hands, feet, arms, or legs is a symptom of reflex sympathetic dystrophy.
- You could get secondary osteoarthritis in your wrist. Pain and swelling in the malformed joint are among the symptoms.
- The tendon tear in the Extensor Pollicis Longus (EPL). Your thumb does not fall on your palm thanks to the EPL tendon
Prognosis
The prognosis for a Colles fracture depends on the extent of the injury and the severity of any aftereffects. Complications can be avoided with early and adequate reduction, casting, splinting, and follow-up care from an orthopedist. For serious injuries such as open fractures, injuries with neurovascular compromise, or compartment syndrome symptoms, orthopedic consultation is required right away.
Surgery is frequently necessary to treat serious damage. The prognosis is also influenced by the patient’s age; younger people are more likely to benefit from bone remodeling, whilst older patients are less likely to do so.
FAQs
What joint is a Colles fracture?
Distal radius fractures with dorsal displacement combine to form Colles fractures, which are among the most frequent wrist injuries.
Why is it called Colles fracture?
Abraham Colles (1773–1843), an Irish surgeon from Kilkenny, is credited for describing the Colles fracture for the first time in 1814 by only observing the typical deformity in the absence of X-ray technology. The first person to use X-rays to investigate it was Ernest Amory Codman.
What structures are damaged in Colles fracture?
Wrist injuries most commonly occur from a Colles fracture. Usually, it happens when a hand that is outstretched falls. The distal section of the radius is fractured by the force of the fall and is displaced into the standard “silver fork” posture.
What is the case of Colles fracture?
A Colles fracture, which is typically associated with a distal forearm “silver fork” or “dinner fork” deformity, is typically caused by falling onto an outstretched hand (FOOSH). They are more common in women who have osteoporosis and in older people.
Where is a Colles fracture located?
A break in the radius at the wrist is called a Colles fracture. It was given the surgeon’s name who originally described it. The break is usually seen approximately one inch (2.5 cm) below the wrist’s joining point.
References
- Colles wrist fracture – aftercare: MedlinePlus Medical Encyclopedia. (n.d.). Colles Wrist Fracture – Aftercare: MedlinePlus Medical Encyclopedia. https://medlineplus.gov/ency/patientinstructions/000896.htm
- Summers, K., Mabrouk, A., & Fowles, S. M. (2023, July 31). Colles Fracture – StatPearls – NCBI Bookshelf. Colles Fracture – StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK553071/
- Colles Fracture. (n.d.). Physiopedia. https://www.physio-pedia.com/Colles_Fracture
- The Basics of a Broken Wrist. (2022, November 12). WebMD. https://www.webmd.com/a-to-z-guides/colles-fracture
- C. (n.d.). Colles Fracture: Symptoms, Causes & Treatment. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/21860-colles-fracture




2 Comments