
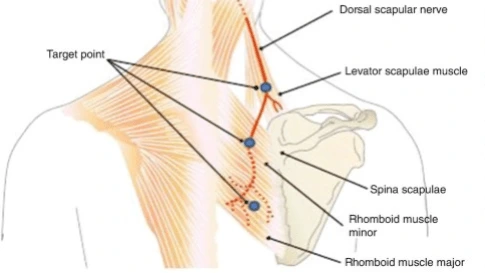
Dorsal scapular nerve entrapment syndrome
What is Dorsal scapular nerve entrapment syndrome?
Dorsal Scapular Nerve Entrapment is the irritation or impingement of the dorsal scapular nerve in your midback. It is an under-recognized cause of upper back, neck, and shoulder edge pain. The symptoms of it frequently overlap with other diseases and can be mistaken for cervical disc herniation, rib ache, or shoulder pathology.
Symptoms of Dorsal scapular nerve entrapment syndrome
- People with dorsal scapular nerve entrapment especially complain of aches over the medial border of the scapula.
- People may also experience interscapular aches, weakness of arm abduction, shoulder, and arm aches, and/or winged scapula.
- They may complain of stabbing, sharp, burning, or knife-like medial scapular ache, neck and back dull ache, lateral arm and forearm ache, and a feeling of traction within the shoulder.
- If dorsal scapular nerve dysfunction is chronic, there may be rhomboid or levator atrophy.
- The beginning of the ache can be sudden or develop gradually over time.
- There may be a record of overhead work or overhead sports.
- Though dorsal scapular nerve entrapment is considered fairly infrequent, it may be much underrecognized, and it may be mistaken with or contained with long thoracic nerve entrapment.
- There may be simultaneous anterior chest wall ache and tenderness over the sternocostal edge, frequently with badly localized ipsilateral arm ache that may be greatly more noticeable than the interscapular ache.
- Dorsal scapular nerve entrapment can present as an atypical thoracic outlet syndrome.
Differential diagnosis
Because the dorsal scapular nerve is frequently overlooked as a diagnosis, most people with dorsal scapular nerve entrapment have been misdiagnosed before the correct diagnosis. Differential diagnosis contains:
- Shoulder pathology: adhesive capsulitis, impingement, rotator cuff arthropathy, AC joint or junctions arthritis
- Cervical radiculopathy
- Thoracic spine pathology: disc protrusion, spondylosis
- Myofascial pain
Diagnosis
- Damage/entrapment of the dorsal scapular nerve induces weakness of the levator scapulae muscle and the rhomboid muscles and outcomes in a winging of the scapula.
- [Scapular winging guides to the irregular protrusion of the scapula on the person’s back. It happens because of paralysis of stabilizing muscles of the scapula. Serratus anterior and trapezius are familiar causes whereas rhomboid weakness is an unusual cause.
- The scapular winging in dorsal scapular nerve syndrome is not as extreme as seen with the serratus anterior muscle and trapezius muscle.]
- The typical complaint in dorsal scapular nerve entrapment is a record of the abnormal motion of the shoulder joint or junction, and stiff joint or junction. The person may also complain of aches in the shoulder area.
- On analysis, as mentioned before, there could be scapular winging. The scapula may evolve laterally displaced with an upward movement.
- When requested to obtain the scapulae together [adduct], the person is not capable to do so or the involved side is less adducted. Palpation of the contracted rhomboid muscles would verify the weakness.
- When the person is asked to push the arm forward on elevation will result in the medial border of the scapula being raised and dragging on the inferior angle of this bone.
- An electromyogram would assist in the verification of diagnosis.
- MRI scan allows for a diagnosis of root avulsions.

Treatment of Dorsal scapular nerve entrapment syndrome
Conservative management
Conservative therapy concentrates on decreasing secondary muscle pressure and on enhancing posture. Non-pharmacological therapies like TENS and acupuncture can be attempted.
Pharmacological treatment
Anti-neuropathic medications like tricyclic antidepressants and antiepileptics (pregabalin, gabapentin) can assist to reduce the symptoms.
Local steroid block for muscle
Dorsal scapular nerve block
Infiltration of local anesthetic and steroids near the dorsal scapular nerve can be diagnostic and therapeutic as well. The injection is conducted under real-time ultrasound recommendation for greater accuracy and security. The nerve can be targeted in the neck as in access via the middle scalene muscle or the posterior thorax as it gives under the Rhomboids.
Because of the notable variability in the anatomy of the nerves and muscles in this highly vascular region of the neck, ultrasound advice is especially helpful for dorsal scapular nerve injections.
Dorsal scapular nerve ablation (Pulsed radiofrequency treatment)
Pulsed radiofrequency lesioning of the dorsal scapular nerve is shown in a person who demonstrates a positive reaction to the diagnostic dorsal scapular nerve block. This approach can ease symptoms associated with dorsal scapular nerve entrapment on a long-term base. The process is conducted under real-time ultrasound advice and the dorsal scapular nerve is ablated at 42 C for 480 seconds.
Botox injection for dorsal scapular nerve entrapment
Injection of botulinum toxin in the rhomboid muscles can ease the symptoms associated with dorsal scapular nerve entrapment.
Physiotherapy treatment
Therapy usually is conservative which contains:
Cervical stabilization
Cervical collar
Cervical traction
Strengthening of the trapezius [middle trapezius gives compensation for loss of rhomboids]
Shoulder blade squeeze
The shoulder edge squeeze is an effortless way to do that.
Stand erect with a good stance.
Gradually press the shoulder edges together and maintain for 3 seconds.
Gradually release the shoulder edges back to their loose positions.
This activity can also be done using a resistance band, cables, or maintaining your arms out front in an ideal post position.

Shrug
Easy shrugs are another method to maintain your trapezius strong. The shrug is very familiar and comfortable to execute, and it’s one of the best activities to activate the trapezius. For an extra challenge, do this activity with weights in your hands.
Stand up erect with a good stance.
Lift your shoulders as elevated as you can get them as if trying to adjoin your ears with your shoulders.
Keep for a count of two.
Dismiss them back into their comfortable positions.
Recount 20 times.

Upright row
This is a popular activity for boosting the trapezius. You can even attempt this with dumbbells or a barbell in your hands.
Stand up straight.
With your fists grasped, drag up your fists as tall as you can while flexing your elbow joints, maintaining your hands close to the front of your body.
Maintain a count of two.
Dismiss your arms back into a comfortable position, fists still grasped.
Recount 20 times.

Pushup
There are a few additional variations of the pushup. Accomplish the version that’s most comfortable for you: A standard pushup, a pushup while kneeling on the bottom or a standing pushup opposite to a wall.
Place your hands flat on the bottom of the wall.
Decline your body toward your hands while maintaining your back straight and your stomach tense. Do not allow your head to fall; maintain your neck in line with the suspension of your spine.
Decline your body until you’re close to the bottom of the wall, and then push back into an erect position. Inhale when you move down and exhale when you move up.
The key to the pushup is to focus on pushing the shoulders together during the activity. Assemble your middle and lower trapezius work to accomplish the job.

Prone lateral raise
Lie flat on your stomach in a prone position on a carpet or bench. Grab a lightweight dumbbell in your hand. Put your forehead on the carpet. Maintain your feet shoulder-width separated. Maintain your arms extended and fully relaxed. Your palms should front in toward your body. This is your beginning position.
Raise your arms to your sides until your elbow joints are at shoulder height and your arms are similar to the bottom. Exhale. Maintain your arms perpendicular to your torso and fully extended via the motion.
When you’ve gained shoulder height, press your shoulder edges together and maintain for one count. Solely your arms should be raised, nobody else. The purpose is to isolate your upper back.
Inhale, then gradually lower the dumbbells back down to the beginning position. Recount 8 times.

Front raise thumbs up
Lie down on your stomach in a prone position on a carpet or bench with your forehead relaxing down. Maintain your feet shoulder-width separated. Have your arms directly out above you, fully relaxed, with your thumbs up in the atmosphere. This is your beginning position.
Exhale and then lift your arms straight. Maintain them fully extended without raising your head off the carpet. This is rigorously a shoulder and upper-back activity, so maintain your torso and lower body glued to the carpet.
Press the muscles between your shoulder edges as you raise as tall as you can without breaking form. Maintain this position for one count.
Inhale and gradually decline yourself back down to your beginning position with your arms fully relaxed. Recount 15 times.

Scapular retraction
Use a Smith device or an assisted pull-up device for this activity.
Have a seat on the bottom in a long sitting position and have your chest directly under the bar. Put your feet shoulder-width separated and flex your knee joints at a 90-degree angle.
Commit your core and hold the bar with your palms meeting far from you. Drag yourself up, maintaining your torso, shoulders, hips, and knee joints in one straight line. This is your beginning position.
With your chest open, press your shoulder edges together by pushing them down and back until you visibly lift yourself to the bar about 2 to 3 inches. Don’t row or drag yourself up. Maintain this retraction for one count.
Maintain breathing, remove the contraction, and arrive back to your beginning position. Recount 15 times.

Scapular wall slides
Lean up opposite a wall. Maintain a tilt in your pelvis so there’s no arc in your back. Your back, head, and buttock should be pushed firmly as opposed to the wall. Exit a slight arch in your knee joints so your legs aren’t completely locked. Completely extend your arms directly above you with your palms facing far from the wall. This is your beginning position.
With your chest open and back elevated, press the muscles of your midback as you glide your arms down toward your shoulders. Maintain your back and the backs of your wrists, palms, and elbow joints pushed up opposite to the wall. You should sense a squeeze right out.
Save in mind, this activity is hard if you’re tight or have poor posture. End when your elbow joints are barely lower than shoulder height.
Maintain this position for one count. Inhale and then force your arms back up to your beginning position without anything raising off from the surface. Recount 15 times.

Neck Flexion Stretch
Begin in a normal position, chin elevated and shoulders lowered.
Gradually lower the head forward by obtaining your chin toward your chest
You should sense a mild pressure up the back of the neck
To raise the stretch, obtain either arm over your head, hold the back of the head with your hand, and slightly drag the head from behind
Lateral Neck Flexion Stretch
Sit or stand with your head in a normal position. Maintain your chin elevated and lower your shoulders
Gradually lower the right ear towards the right shoulder, being mindful not to raise the opposite shoulder
You should sense a mild pressure on the side of your neck
To raise the stretch, obtain your right arm up and over your head. Hold the left side of your head and slightly drag it toward your opposite shoulder
Head Swings
Sit or stand with your head in a normal position. Maintain your chin elevated and lower your shoulders
Gradually lower head toward chest, and then slightly move the right ear to the right shoulder
Obtain the head back to normal position, and recount on the further side
Head Rolls (Cervical Spine Rotation)
Sit or stand with your head in a normal position. Maintain your chin elevated and lower your shoulders
Gradually and slightly move the head in a clockwise loop three times.
Recount in the opposing direction
The strengthening happens during rotation when the head moves from front to back
Surgery
Surgery can be viewed in extreme cases that are unresponsive to conservative therapy.
The methods are:
Fascial sling operation
Two fascia lata grafts are used to attach the lower medial wall of the scapula to the spinal muscles and the inferior tip of the scapula to the latissimus dorsi muscle.
This anchors the scapula to the posterior thoracic wall, stopping winging.
Grafts may lengthen or die with time
Neurolysis or nerve decompression
Presented as a last resort
FAQ
What does dorsal scapular nerve entrapment feel like?
They may complain of stabbing, sharp, burning, or knife-like lateral arm and forearm pain, medial scapular ache, neck and back dull ache, and a feeling of traction within the shoulder. If dorsal scapular nerve dysfunction is chronic, there may be rhomboid muscle or levator muscle atrophy. The beginning of the ache can be sudden or develop gradually over time.
What happens if a dorsal scapular nerve is damaged?
Dorsal scapular neuropathy may result in irregular movement of the shoulder joint or junction with scapular winging. Dorsal scapular neuropathy is irregular and may influence shoulder impingement or rotator cuff injury. Thus, it is hard to determine the correct diagnosis of scapular winging established on physical inspection.
Is nerve entrapment permanent?
While ulnar nerve entrapment is generally not serious, it can have permanent effects without prompt therapy, involving paralysis and loss of sensation in the involved hand or arm. Yet, with accurate diagnosis and therapy, most patients with ulnar nerve entrapment can make a complete recovery.
What causes dorsal nerve damage?
It is generally the result of damage or infection. When swelling causes stress on a nerve, the myelin sheath wrapping the nerve may be injured. The nerve may also evolve trapped or squeezed. Nerve ischemia (deficiency of oxygen to the nerve) can also cause harm.
How long does it take the dorsal nerve to heal?
Regeneration time relies on how seriously your nerve was damaged and the kind of injury that you maintained. If your nerve is discolored or traumatized but is not cut, it should heal over 6-12 weeks. A nerve that is cut will expand at 1mm per day, after almost 4 weeks of ‘rest’ following your damage.



2 Comments