Hemiepiphysiodesis
What is a Hemiepiphysiodesis?
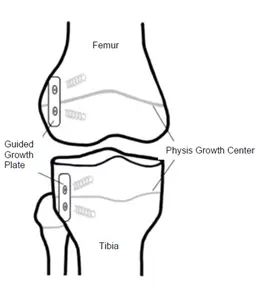
Hemiepiphysiodesis is a surgical procedure performed on growing bones to correct angular deformities, typically in the long bones of the legs, such as the femur and tibia. This procedure involves the partial growth plate arrest, which aims to guide the growth of the bone in a more desirable direction, thereby correcting the angular deformity.
The growth plate, also known as the physis, is the area of developing tissue near the ends of the long bones in children and adolescents. It is responsible for the lengthening of bones during the growth period. By partially restricting the growth plate on one side of the bone, the procedure allows the other side to continue growing, which can gradually straighten the bone.
Temporary hemiepiphysiodesis is reversible, meaning that the growth plate can return to normal development and function once the needed correction is made by removing the metal implants used to create epiphysiodesis. On the other hand, following surgery, persistent epiphysiodesis cannot be reversed and growth plate function cannot be recovered.
Paediatric orthopaedic diseases are treated with both temporary hemiepiphysiodesis and permanent epiphysiodesis; however, there are differences in the specific indications for each treatment.
Guided growth temporary hemiepiphysiodesis
A common treatment for children’s angular or coronal plane abnormalities at the knee, such as genu varum or genu valgum deformities that occur in the medial/lateral plane, is temporary hemiepiphysiodesis. It has also been used to correct abnormalities originating from the anterior/posterior plane, or sagittal plane deformities. Additionally, anomalies in the growth plates of the upper limbs, such as the distal radius growth plate, and around the hips and ankles have been treated using temporary hemiepiphysiodesis.
The mechanism of temporary hemiepiphysiodesis involves stopping or impeding the growth of one hemi-side of the growth plate. As a result, the opposite hemi-side is let to grow freely and normally. In most situations, this procedure proceeds gradually and steadily until the angular distortion is corrected.
Children with a variety of bone and joint conditions, including rickets, Blount’s disease, osteochondrodysplasias, arthrogryposis multiplex congenital, idiopathic, trauma, and renal osteodystrophy, have had their angular deformities treated with temporary hemiepiphysiodesis or guided growth surgery.
A more straightforward and effective substitute for the traditional, time-honored osteotomy or bone-cutting procedure is temporary hemiepiphysiodesis. Whereas temporary hemiepiphysiodesis corrects deformities gradually, bone osteotomy corrects them instantly. For guided growth surgery or temporary hemiepiphysiodesis, a range of metal implants, such as a two-hole plate with screws and staples, have been applied.
Once the desired deformity correction has been achieved, any metal implants that were initially utilized to induce temporary hemiepiphysiodesis should be removed. Should this not happen, the kid will have overcorrection, or the reverse malformation. For instance, if a kid receiving treatment for a genu varum deformity has their metal implant removed prematurely, it may lead to overcorrection of the genu valgum deformity and vice versa.
Hemiepiphysiodesis Technique
- A surgical procedure called hemiepiphysiodesis, or directed growth, is used to gradually treat angular limb deformities in individuals with immature skeletons.
- This surgical procedure has less side effects, a shorter immobilisation period, lower costs, and a lower surgical risk than corrective osteotomies.
- Premature epiphyseal closure, a rebound period of increased development, or hardware migration might complicate temporary hemiepiphysiodesis performed by plating or stapling; difficulties seem to be lesser when applying the extraperiosteal, 2-hole plate approach.
- 2-hole plates with parallel screw configurations seem to be more effective than divergent screw designs in inhibiting development, while being the subject of debate in the literature. It has not been demonstrated that the screw and plate sizes influence the angular correction rate.
Description
Growing periods aggravate children’s and teenagers’ activity-related pain, altered gait mechanics, and joint instability resulting from pathological angular deformities of the lower limbs. By conducting permanent hemiepiphysiodesis with physical ablation or temporary hemiepiphysiodesis with Blount staples (Blount, 1945) or a tension band plate (Stevens, 2007) across one side of the physis, angular abnormalities can be gradually repaired with growing.
Without destroying any physis or requiring extensive surgery, the patient may typically achieve equal leg lengths, neutral mechanical axes, and horizontal knees by skeletal maturity through directed development. Temporary hemiepiphysiodesis permits the complete physis to continue growing following device removal, in contrast to ablation of the physis. It takes precise timing and surgical expertise to prevent overcorrection or undercorrection.
Indications
One of our surgical professionals will evaluate candidates to make sure a correct diagnosis is made and all physical requirements are met.
For limb-lengthening procedures, we treat patients of all ages. Throughout the whole process of limb lengthening, patients, and in certain circumstances their carers, must be willing to engage in physical therapy and make many consultations with their physician.
Suitable candidates with this procedure’s experience include:
- Limb deformity affecting multiple planes
- length disparity between two appendages
- combination of length disparity and deformity
- soreness in their knees, ankles, hips, back, posture, and hips
- greater intensity of pain on one side of the body
- The problem with walking or gait
Outcomes
In general, guided growth surgery and temporary hemiepiphysiodesis yield good outcomes. Compared to external fixation correction or osteotomy, this surgical technique is thought to be less stressful and safer. In general, the problems have a low profile in terms of frequency and severity. However, there are issues with the use of temporary hemiepiphysiodesis in conditions such osteochondrodysplasias and Blount’s disease.
Blount’s disease has been directly linked to mechanical failure of the metal implant, such as the plate and screws, and failure to accomplish full rectification of the deformity. Furthermore, recurrent operations and the rebound phenomenon, which is the return of bone abnormalities, have been strongly associated with bone deformities resulting from osteochondrodysplasias. In general, when the metal implant used to repair the deformity is removed, children should be monitored for rebound or return of the deformity.
Permanent epiphysiodesis
Outcome and complications
In order to ensure that the patient’s limbs are almost equal in length by the time their skeletal growth ends, the treatment needs to be carried out for the right amount of time throughout their teenage growth phase. A length mismatch brought on by inadequate scheduling can have significant adverse effects on patient outcomes and morbidity.
Potential complications
Epiphysiodesis is a surgical treatment that might provide challenges and problems like any other. We take great precautions to prevent issues and teach patients how to take good care of their bodies while undergoing treatment, all the while teaching them about these possible hazards. Our team of professionals is prepared to handle any issues that may develop. Side effects and complications might include:
- Angular malformation is caused by the growth plate closing partially or asymmetrically
- Fracture of the growth plate
- Permanent growth plate injury
- Joint injury
- The rebound phase of the rapid growth following the removal of an 8-plate
- Iatrogenic limb length inequality
- Overcorrection or undercorrection
- Hardware migration
Pre-operative care
- On the first evaluation, a thorough medical history of your kid will be obtained.
- It might be necessary to cease using some supplements and prescription drugs several weeks prior
- Talk to your surgeon about any prescription and over-the-counter medications.
- To keep track of your child’s pre- and post-operative appointment dates, use an agenda or calendar.
- Make plans to support your kid during the guided development phase and after surgery.
Post-operative care
- As the patient tolerates it, early mobility and activity are advised.
- Three to five days following surgery, the huge compressive elastic bandages can be taken off. The tiny adhesive dressings, however, need to stay in place and dry until your initial follow-up visit.
- As soon as they feel comfortable, your kid who has an epiphysiodesis can begin to partially bear weight on the injured limb with crutches.
- Your child will be able to bear their entire body weight and just use crutches for comfort if they have a hemi-epiphysiodesis.
- Maintaining strength and range of motion will require physical therapy in order to resume regular activities.
- Following surgery, it’s critical to keep an eye on your child’s suffering. Over-the-counter pain relievers are advised for the first week.
- If the pain is more severe, we could recommend a little dose of painkillers.
- When you’re sleeping, use pillows and other comfort measures as required. Raise your leg to lessen swelling.
Follow-ups after surgery
- After surgery, your kid will have their first follow-up in 7 to 14 days to have their incisions examined and coverings taken off.
- Radiograph follow-up is advised every three to six months.
- After directed growth is completed, it is crucial to schedule follow-up appointments with your surgeon since, without the plates, the legs would continue to straighten and eventually distort in the opposite way.
- After complete rectification, the hardware is removed.
- Intermittent follow-up should last for at least a year and a half, depending on age.
- Follow-ups may be required once the correction is complete in order to keep an eye on your kids as they develop.
Overview
Leg length variations might impact a child’s activities or result in unequal joint wear. A method called epiphysiodesis can be used to temporarily or permanently regulate a bone’s development. Growth plates are present in all of the long bones in the lower limbs.
By focusing on one or more of these growth centres, our surgeons can specifically impede or cease a bone’s development. Instead of producing effects right once, epiphysiodesis progressively corrects disparities in limb length over time. One limb’s slower growth allows the other limb’s leg length disparity to adjust over time.
Hemi-epiphysiodesis, often known as directed growth, is a method that slows or stops one-half of the growth plate. This method is applied to angular abnormalities such as genu varum or genu valgum (bowed legs or knock knees) to cure the deformity by slowing the growth of one leg and promoting quicker growth on the other. An 8-plate, or tiny plate with two holes. It is usually placed on either side of the growth plate in order to facilitate directed development.
FAQs
How is Hemiepiphysiodesis done?
For this minimally invasive procedure, the kid or teenager is usually put under general anaesthesia for less than an hour. A 1-inch (2.5-cm) incision is created, and either a Métaizeau screw or a tension-band plate that crosses the growth plate is introduced and fastened with bone screws.
What are the different types of Hemiepiphysiodesis?
Epiphysiodesis comes in two types: temporary hemiepiphysiodesis and permanent epiphysiodesis. Targeted growth or growth flexion surgery is another term for temporary hemiepiphysiodesis.
What are the complications of Hemiepiphysiodesis?
These include inadvertently incomplete epiphysiodesis effect necessitating repeat surgery, wound hematoma, postoperative hemarthrosis with or without associated knee stiffness, superficial or deep infection, temporary or permanent neuropathy, and inaccurate surgery timing resulting in under- or overcorrection of LLD.
What are the methods of epiphysiodesis?
Surgical techniques for epiphysiodesis vary widely. To stop the bone from expanding, surgeons have three options: they can drill the growth centre, put screws across it, or tether each side of it with a tiny plate.
What is the recovery time for Hemiepiphysiodesis surgery?
After surgery, the patient is able to bear weight on the leg right away. After two to three weeks, they can resume their regular activities. Three weeks should be spent away from contact sports. Physical therapy is advised for a few weeks following surgery. It is to minimize stiffness since there may be some edema in the knee.
References
- Epiphysiodesis and Hemiepiphysiodesis (2023, April 3). CLLC, Canadian Limb Lengthening Center https://cllcenter.com/procedure/epiphysiodesis-and-hemiepiphysiodesis/
- Epiphysiodesis. (2023, August 17). Wikipedia. https://en.wikipedia.org/wiki/Epiphysiodesis
- Hemiepiphysiodesis Technique | Pediatric Orthopaedic Society of North America (POSNA). https://posna.org/physician-education/study-guide/hemiepiphysiodesis-technique