

Hypothenar Hammer Syndrome
What is a Hypothenar Hammer Syndrome?
Hypothenar hammer syndrome is a condition of the palm in which the blood supply (mainly the ulnar artery) of the palm is decreased. Hypothenar refers to the group of muscles that determine the movements of the little finger. Some of these muscles make up the bulky edge of the palm (hypothenar eminence).
Hypothenar hammer syndrome (HHS) is affected by repeated use of the heel of the palm or palm as a mallet(hammer), it causes thrombosis(blood clot) of the superficial palmar arch of the ulnar artery. There is injury over the hook of the hamate, where the superficial branch of the palmar artery lies down. This causes vascular lack of the ulnar side of the hand.
Epidemiology of Hypothenar Hammer Syndrome
Hypothenar hammer syndrome (HHS) is likely rare but may be underdiagnosed.
Generally, it happens in men more than women at age around 40 years, in professions and sports where the heel of the hand is operated as a mallet or is subject to repeated force; for example:
- Professions such as metal workers, mechanics, machinists, sawmill workers, miners, carpenters, butchers, bricklayers, bakers, and those using vibrating devices in their work.
- Different sports involve golf, mountain biking, baseball, softball, hockey, and martial arts.
Causes of Hypothenar Hammer Syndrome
It happens when people frequently use the hypothenar eminence of the hand as a mallet to push, grind, and twist tough things. These movements can hurt specific blood vessels of the hand, mainly the ulnar artery. This artery runs via the hypothenar area of the hand and supplies blood to the fingers. Impairment to the ulnar artery effects in a deduction of blood flow to the fingers. Sometimes a single important attack can provoke hypothenar hammer syndrome.
Likely factors involved in causation are:
- Single or repeated impacts to the heel of the hand
- Pre-existing irregularities of the arteries or deviations in arterial anatomy (eg incomplete superficial palmar arch)
- Following prothrombotic aspects
- Other anatomical deviations, for example, an anomalous hypothenar muscle.
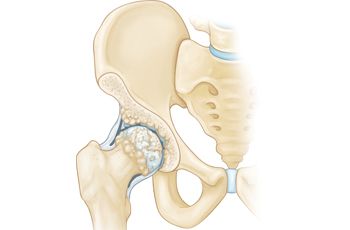
Anatomy and Pathophysiology of Hypothenar Hammer Syndrome
The ulnar artery is weak in the distal part of Guyon’s canal, which is not covered by the palmaris brevis muscle. Guyon’s canal is a concave space between the pisiform and hook of the hamate that is altered into a fibro-osseous tunnel by the pisohamate ligament. At this spot, the superficial branch of the ulnar artery can be squeezed against the bony hook of the hamate.
Repetitive direct trauma may lead to arterial impairment, thrombus formation, aneurysm of the artery, or microemboli, leading to digital ischemia.
Sensory components of the ulnar nerve run nearby and their involvement can cause symptoms of hypothenar hammer syndrome.
Symptoms of Hypothenar Hammer Syndrome
- Cold sensation and pain in the palm
- Raynaud syndrome
- Tender hypothenar eminence
- Ischemia of (usually) fourth and fifth fingers
- Positive Tinel sign due to ulnar nerve compression in palm

Diagnosis of Hypothenar Hammer Syndrome
Physical examination conclusions of HHS contain tenderness at the hypothenar eminence, lack of the ulnar pulse, and positive Allen’s test in the involved hand. Duplex ultrasound is a proper first test, and the gold standard for diagnosis is angiography.
Angiography (DSA) may saws:
- “corkscrew” or beaded weird impression distal ulnar artery
- Aneurysm formation
- Occlusion of the ulnar artery part overlapping the hook of the hamate
- Occluded or under-filled distal digital arteries in an ulnar artery allotment
Positive Allen test: Allen’s test estimate the patency of the superficial palmar arch. The test is performed as follows:
- The patient sits with their hands supinated over the knees.
- The examiner squeezes the radial and ulnar arteries by using his thumbs.
- The patient opens and closes their fist rapidly for several periods, to exsanguinate the hand, be careful not to exceed the fingers.
- The ulnar artery is released; normal color should return in the palm within 5 seconds. If the ulnar artery is blocked, the color will return in the palm just on the release of the radial artery. This indicates a ‘positive Allen’s test’.
- A positive Allen test means obstruction or insufficient development of the superficial palmar arch or distal ulnar artery. However, false positives and false negatives are using Allen’s test.
Differential Diagnosis of Hypothenar Hammer Syndrome
Hand-arm vibration syndrome
Raynaud’s phenomenon from other causes. Features that difference between hypothenar hammer syndrome (HHS) and classical Raynaud’s are:
- The male preponderance and occupational history
- Allen’s test
- Lack of the usual hyperaemic flush phase of Raynaud’s phenomenon
- Digital ulcers in an area supplied by the affected vessel
- Reduced ulnar/radial pulse
Treatment of Hypothenar Hammer Syndrome
The treatment of HHS begins by avoiding those actions that induced the syndrome. Other treatments may contain smoking cessation (smoking affects blood circulation), the use of padded defensive gloves, and avoiding the cold. Specific drugs will allow for the restoration of blood flow.
Medical treatment
- Avoidance of cold.
- Possible drug treatment contains calcium channel blockers, vasodilators and platelet inhibitors, pentoxifylline, and anticoagulation.
- Treat the following atherosclerotic and prothrombotic factors, for example, smoking cessation and lipid management.
- Proteinase has been used to clear an obstruction, as has prostaglandin E1 with heparin.
Exercises for Hypothenar Hammer Syndrome
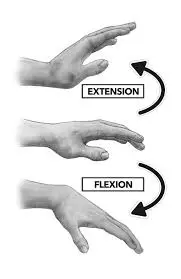
Wrist flexion and extension: Arrange your forearm on a flat table on a rolled-up towel for padding with your hand swinging off the border of the table, palm must be down.
- Move the hand upward and downward with a gentle stretch at the end ROM.
- Repeat the same movements with the elbow flex at your side, palm facing up.
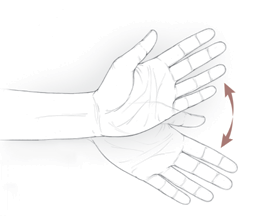
Wrist twisting: Support your forearm on a table or on your knee, thumb must be upward.
Move the wrist upward and downward till its end ROM.

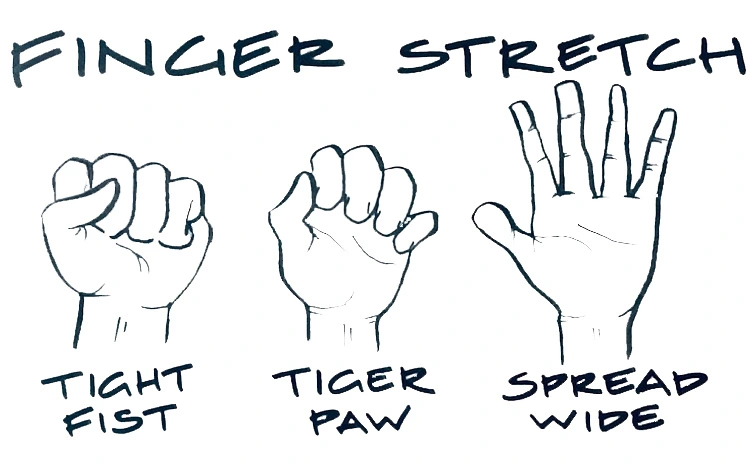
Hand/finger tendon glide: Begin with the fingers spread straight out.
- Make a clenched fist or hook fist; return to a straight of the fingers.
- Make a straight fist or half fist; return to a straight of the fingers.
- Make a full fist(fingers are fully flexed); return to a straight of the fingers.
Finger stretching: Put your hand palm-down over a table or further flat surface.
- Softly straighten your fingers as flat as you can against the surface without pushing your joints on the surface.
- Maintain for 30 to 60 seconds and then remove.
- Repeat four-five times with each hand.

Squeezing: Keep a softball in your affected hand and squeeze it as tough as you can. Maintain for 5 seconds, then release. Do repeat 10 times, and relax for 1 minute.
Finger spreading: Make a soft fist, covering your thumb over your fingers.
- Hold for 30 seconds. Release and extend your fingers wide.
- Do this with affected hands at least 4-5 times.

Surgery
There are different purposes of surgery – to remove an origin of an embolism or a painful mass, to alleviate ulnar nerve compression, or to initiate a local periarterial sympathectomy.
Different surgical procedures may be operated:
- Vascular approaches, for example, ligation, vein graft, or arterial graft.
- Intra-arterial vasodilators or thrombolysis
- Endoscopic thoracic sympathectomy – even though this has been said to give inadequate results.
- There are controversies for and as opposed to surgical treatment as the management of hypothenar hammer syndrome (HHS).
Prevention of Hypothenar Hammer Syndrome
- Smoking cessation
- Avoidance of further trauma
- Padded protective gloves
- Cold avoidance
- Calcium channel blockers (e.g. nifedipine, diltiazem)
- Antiplatelet agents or anticoagulation
- Local care of fingers with necrosis
- Pentoxifylline: for viscosity reduction
Conclusion
The rarity of the hypothenar hammer syndrome generally causes a delayed diagnosis because the syndrome may go undetected for flow compensation through a radial artery and probably is underestimated in hand workers. Therapy methods, in non-symptomatic cases, are observation and risk factor management. In some cases, surgery determined the nerve entrapment generating the pain. At the time of the new thrombosis the surgical approach, in an asymptomatic patient, well managed by drug therapy, is not yet justified.
FAQs
What causes hypothenar hammer syndrome?
Hypothenar hammer syndrome is a moderately occasional disease process induced by repetitive stress or injury to the hypothenar eminence leading to chronic damage to the ulnar artery.
What artery is hypothenar hammer syndrome?
Hypothenar hammer syndrome (HHS) is caused by injury to the ulnar artery either by occupational or sporting activities. The diagnosis should be imagined when a younger male presents with signs of pain, a detectable bulge, and ischemia, in the predominant hand.
What are the 4 hypothenar muscles?
The hypothenar eminence contains four muscles, of which there are mainly three primary muscles. The flexor digiti minimi brevis muscle, the abductor digiti minimi muscle, the palmaris brevis muscle, and the opponens digiti minimi muscle are the four muscles that make hypothenar eminence.
What is the difference between the thenar and hypothenar muscles?
The word thenar arises from the Greek meaning “palm of the hand.” The thenar eminence is located at the radial part of the volar hand at the base of the thumb. The hypothenar eminence is located on the ulnar part of the volar hand at the bottom of the fifth digit (little finger).
What is claw hand?
A claw hand is a condition that induces curved or flexed fingers. This creates a hand that seems like the foot of an animal.


2 Comments