Inferior Oblique Muscle
Introduction
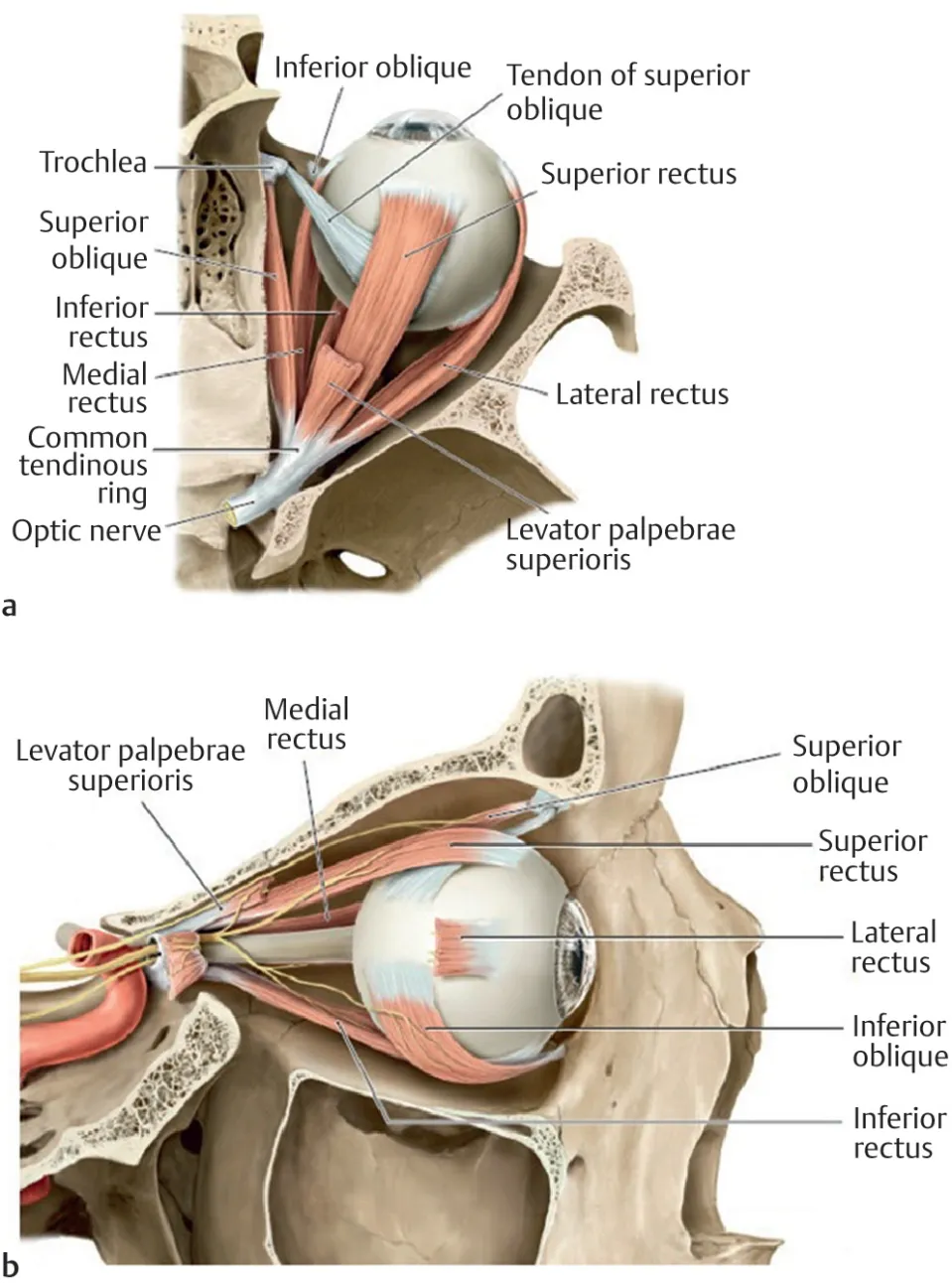
Extraocular muscles are essential for ocular movement. The four rectus muscles, superior oblique muscle, and inferior oblique work in conjunction to move the eyes in every direction. The inferior oblique is a thin, narrow eye muscle and belongs to the group of six extraocular muscles or the orbit’s extrinsic muscles. The inferior oblique muscle is primarily reliable for external rotation. The secondary and tertiary movements are elevation and abduction, respectively.
The inferior oblique muscles are described as having two surfaces; 1. superiorly, the ocular surface, and 2. inferiorly, the orbital surface. At the orbital groove, the muscles are described in terms of their anterior and posterior border. The inferior oblique tendon inserts in the sclera, underneath the lateral rectus.
Embryology
The inferior oblique, along with the superior, inferior, and medial rectus muscles, is emanated from the prechordal mesoderm. A unique quality of the inferior oblique, compared to the superior oblique, is that it is almost completely muscular, rather than both muscular and tendinous.
While commonly affected by palsies of the inferior division of the oculomotor nerve, separated palsies of the inferior oblique (without affecting other functions of the oculomotor nerve) are quite rare.
Origin
Synonyms: Musculus obliquus inferior bulbi oculi
The thin inferior oblique muscle lies around the anterior border of the floor of the orbit. Similar to the superior oblique muscles, but unlike the rectus muscles, the inferior oblique does not originate from the common tendinous ring (annulus of Zinn). Instead, the inferior oblique originates from the anterior aspect of the orbit.
Specifically, from the medial (orbital) surfaces of the maxilla just lateral to the nasolacrimal fossa. From there it ascends obliquely and posterolaterally, running between the lateral rectus muscle and the floor of the orbit. The muscle inserts into the inferolateral half of the sclera, posterior to the equator of the eyeball.
Insertion
The inferior oblique muscle inserts at the posterior quadrant of the eyeball (inferolateral part) between the lateral and inferior recti muscles and slightly posterior to the insertion of the superior oblique muscles. As the inserting tendon of the inferior and superior oblique muscles give each further, they lie in the same oblique vertical plane.
The fascial sheath of the inferior oblique blend with the thickened sheath of the inferior rectus muscles. These two then blend with the medial and lateral inspection ligaments, which are triangular sheet elaborations of the medial and lateral recti muscles. This fusion of the inferior rectus, inferior oblique muscle, and review ligaments, forms the suspensory ligament of the eyeball, a hammock-like sling that supplies assets to the eyeball. Additionally, the fused sheaths of the inferior rectus and inferior oblique pass off an anterior expansion called the inferior check ligament which connects itself to the tarsus of the inferior eyelid.
Nerve supply
The inferior oblique muscles are supplied by the inferior division of the oculomotor nerve (CN III), which delivers it with general somatic efferent fibers.
The nerve to the inferior oblique is the longest branch of the inferior branch of the oculomotor nerve. It joins the muscle through its orbital surface.
The inferior division of the oculomotor nerve also carries parasympathetic fiber along the optic nerve to the ciliary ganglion. These fibers innervated the sphincter pupillae and ciliary muscles.
Blood supply
The inferior oblique is supplied by the ophthalmic artery and infraorbital artery, these arise from the internal carotid and maxillary arteries, respectively.
Function
Its movements are extorsion, elevation, and abduction of the eye.
The primary movement is extorsion (external rotation), the second movement is elevation, and the tertiary movement is abduction (i.e. it exacts the eye and moves it upward and outwards). The area of maximal inferior oblique elevation is in the adducted position.
The inferior oblique muscles are the only muscle that is capable of elevating the eye when it is in a fully adducted position.

Clinical Significance
While commonly affected by palsies of the inferior division of the oculomotor nerve, isolated palsies of the inferior oblique (without involving other functions of the oculomotor nerve) are quite rare.
“Overaction” of the inferior oblique muscles is a commonly observed feature of childhood strabismus, especially infantile esotropia, and exotropia. Because true hyperinnervation is not usually present, this splendor is better termed “elevation in adduction”.
The surgical procedure of the inferior oblique includes loosening (also known as recession see Strabismus surgery) myectomy, marginal myotomy, and denervation and extirpation. It is also discovered and determined in lower lid blepharoplasty surgeries.
Diagnosis of inferior oblique dysfunction is frequently discovered by parents and pediatricians, permitting an early referral to an ophthalmologist. In the earlier stages, patching in the dominant eye can force the eye with the injury to compensate and strengthen. However, later on, the patching techniques may not be successful and surgical intervention is the recommended option.
In lower blepharoplasty resection, the inferior oblique muscles are susceptible to injury. Patients will demonstrate symptoms ranging from transient diplopia to permanent strabismus. Diplopia resulting from an inferior oblique injury usually shows as a distorted visual image with an upward lateral gaze. Patients often unknowingly counteract by tilting their heads or lifting their chins.
Surgical Considerations
The inferior oblique muscles externally rotate, elevate, and abduct the eye. Any injury to these muscles may result in strabismus, which can be an apparent extraocular defect. Though the patient may find methods to compensate for the extraocular movement disability, cosmetic repair requires surgical intervention.
Inferior oblique muscle overaction lives in 70% of patients with esotropia and 30% of patients with exotropia. Overaction is defined as an unnecessary elevation in the eye when attempting to adduct. Inferior oblique overaction separates into two categories; primary and secondary. Primary indicates the patient was born with bilateral inferior oblique overaction, consequently causing infantile esotropia. The secondary type is unilateral and results from a deficiency in the superior oblique muscle. The superior oblique muscle is reliable for abduction, internal rotation, and depression. Hence, if there is paralysis of the superior oblique muscles, the inferior oblique movement is unopposed and results in excessive elevation.
Surgical modification of inferior oblique overaction includes disinsertion, extirpation and denervation, recession, myectomy, and anterior transposition of the muscles.
The anterior transposition procedure of the inferior oblique muscle is a chance for patients who have inferior oblique overaction with dissociated vertical deviation. In this procedure, the inferior oblique muscle gets converted to a depressor. The normal activity of the temporal 14 mm of the muscle contracts was significantly reduced. The posterior part of the inferior oblique is transformed into a depressor, limiting the upward gaze to 30 to 35 degrees.
A myectomy is conducted when a patient shows vertical hypertropia, without dissociated vertical deviation. Patients with inferior oblique overaction are at improved risk for retinal holes and tears. Hence, a myectomy exists as both a prophylactic measure in addition to a cosmetic modification. In inferior oblique overaction, the muscles pull on the thin sclera, and is more reasonable to form a tear or hole in the retina. The inferior oblique muscles are transected and often used to supply traction to the globe during enucleation.
FAQ
Where accomplishes the inferior oblique muscle originate?
The inferior oblique muscle has its origin on the maxillary bone slightly posterior to the inferior medial orbital rim and lateral to the nasolacrimal canal. The inferior oblique is the only extraocular muscle to maintain its anatomic origin in the anterior orbit.
What type of muscle is the inferior oblique?
The inferior oblique muscle or obliquus oculi inferior is a thin, narrow muscle positioned near the anterior margin of the floor of the orbit. The inferior oblique is one of the extraocular muscles and is attached to the maxillary bone (origin) and the posterior, inferior, and lateral surface of the eye (insertion).
What action does the inferior oblique do?
The inferior oblique is reliable for extorsion, elevation, and abduction. Because of their approach, the superior and inferior oblique muscles are the only one muscles that can depress or elevate the eye, respectively when the eye moves in adduction.
What controls the inferior oblique muscle?
The Oculomotor Nerve or Cranial Nerve III. The oculomotor nerve supplies motor innervation to the levator palpebrae superioris, the superior, medial, and inferior rectus muscles, and the inferior oblique muscle.
Is the inferior oblique muscle located in the eye socket?
The inferior oblique is an extraocular muscle that originates in the front of the orbit near the nose. It then travels outward and backward in the orbit before connecting to the bottom part of the eyeball.