
OCULOMOTOR NERVE
INTRODUCTION :
The oculomotor nerve is the third cranial nerve (CN III). It enters the orbit via the superior orbital fissure and innervates extrinsic eye muscles that enable most movements of the eye and that raise the eyelid.
The nerve also contains fibers that innervate the intrinsic eye muscles that enable pupillary constriction and accommodation (ability to focus on near objects as in reading).
The oculomotor nerve is derived from the basal plate of the embryonic midbrain. Cranial nerves IV and VI also participate in control of eye movement.
Overview :
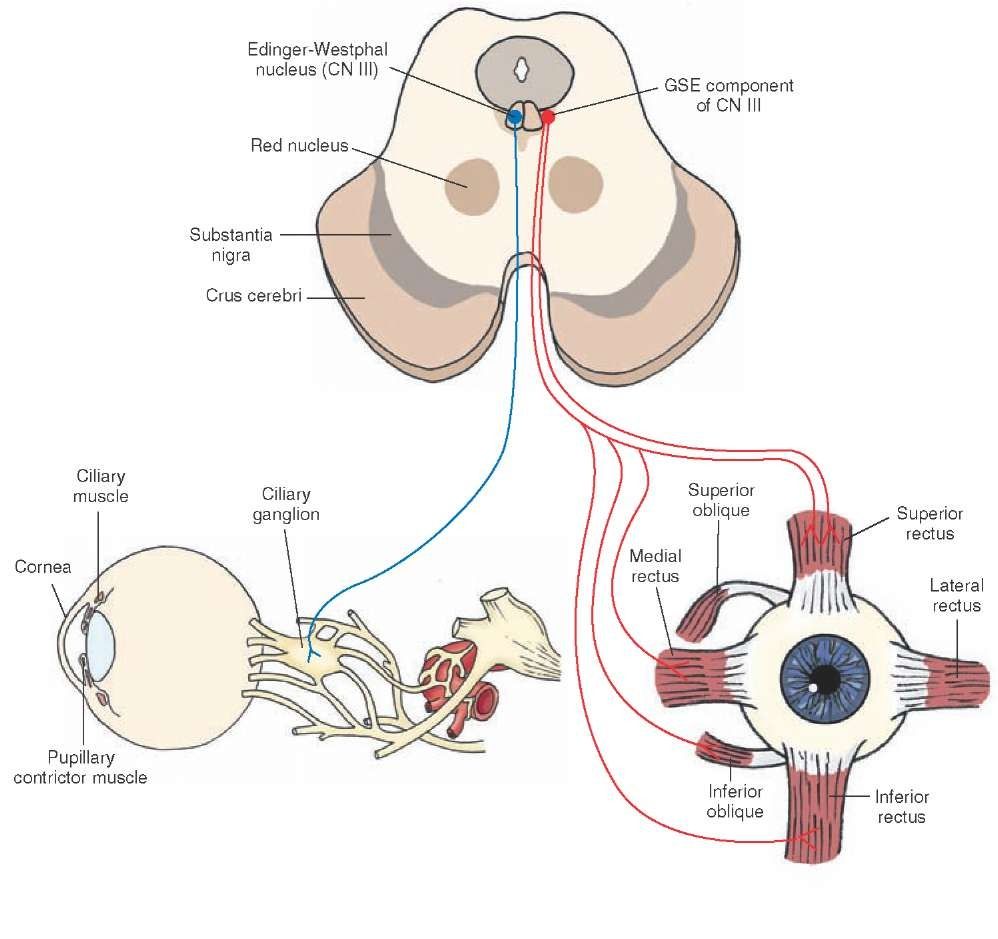
Motor – Innervates the majority of the extraocular muscles (levator palpebrae superioris, superior rectus, inferior rectus, medial rectus and inferior oblique).
Parasympathetic – Supplies the sphincter pupillae and the ciliary muscles of the eye.
Sympathetic – No direct function, but sympathetic fibres run with the oculomotor nerve to innervate the superior tarsal muscle (helps to raise the eyelid).
Anatomical Course :
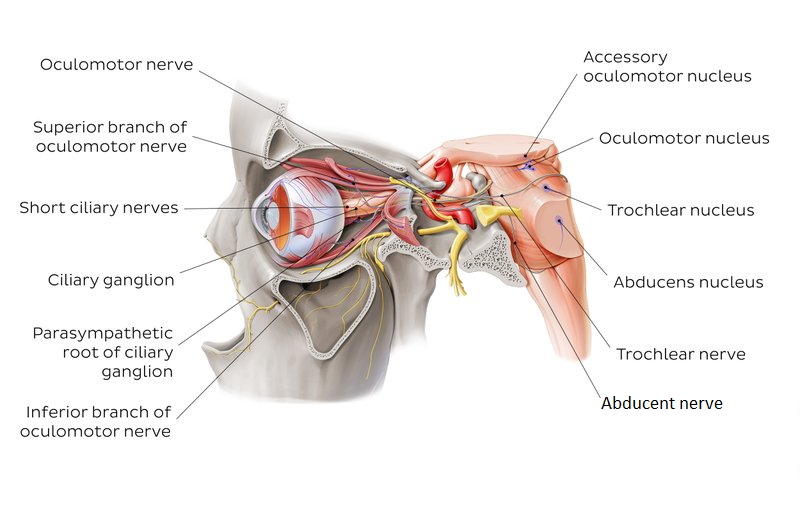
The oculomotor nerve originates from the oculomotor nucleus – located within the midbrain of the brainstem, ventral to the cerebral aqueduct.
It emerges from the anterior aspect of the midbrain, passing inferiorly to the posterior cerebral artery and superiorly to the superior cerebellar artery.
Nerves :
The oculomotor nerve helps to adjust and coordinate eye position during movement. Several movements assist with this process:
- Saccades, smooth pursuit, fixation, accommodation, vestibulo-ocular reflex, and optokinetic reflex.
- Saccades are rapid, jerky motions of the eye. This type of motion typically occurs when moving a gaze between objects.
- When tracking an object, we use smooth pursuit to keep our eyes focused on an object as it moves.
- When we want to stare at an object, we fixate on that object. Control of each of these actions is by either vestibule-ocular or optokinetic reflexes.
- The vestibule-ocular reflex adjusts eye position during fast movements of the head. Head motion activates cells within the semicircular canals.
- Information about the motion is transmitted to the ipsilateral vestibular nucleus and forwarded to the oculomotor nucleus.
- Therefore, if the head moves to the left, the eyes move to the right to keep the gaze steady.
- The optokinetic reflex adjusts eye position in response to changes in the visual field. This reflex initiates from visual information.
- Information about the visual field is transmitted from the parieto-occipital eye field through the pontine nuclei to the vestibule-cerebellum.
- It then moves through the vestibular nuclei to the oculomotor nucleus where eye movement initiates. This reflex allows the eyes to follow large objects in the visual field.
- The last action is accommodation. This action helps to keep the gaze focused with both vestibular and visual stimuli change.
- The nerve then pierces the dura mater and enters the lateral aspect of the cavernous sinus. Within the cavernous sinus, it receives sympathetic branches from the internal carotid plexus.
- These fibres do not combine with the oculomotor nerve – they merely travel within its sheath.
- The nerve leaves the cranial cavity via the superior orbital fissure. At this point, it divides into superior and inferior branches:
- Superior branch – provides motor innervation to the superior rectus and levator palpabrae superioris.
- Sympathetic fibres run with the superior branch to innervate the superior tarsal muscle.
- Inferior branch – provides motor innervation to the inferior rectus, medial rectus and inferior oblique.
- Also supplies pre-ganglionic parasympathetic fibres to the ciliary ganglion, which ultimately innervates the sphincter pupillae and ciliary muscles.
Muscles :
The oculomotor nerve controls several muscles:
- Levator palpebrae superioris – raises the upper eyelid
- Superior rectus muscle – rotates the eyeball backward, “looking up”
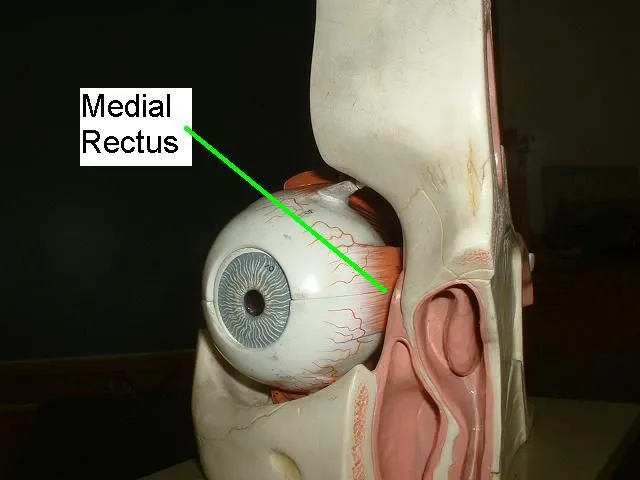
- Medial rectus muscle – adducts the eye, “looking towards your nose”
- Inferior rectus muscle – rotates the eyeball forwards, “looking down”
- Inferior oblique muscle – rotates the eyeball backward when the eye is adducted
- Ciliary muscle – controls lens shape to focus on up-close objects
- Sphincter pupillae – constricts the pupil
Motor Functions :
The oculomotor nerve innervates many of the extraocular muscles. These muscles move the eyeball and upper eyelid.
Superior Branch :
- Superior rectus – elevates the eyeball
- Levator palpabrae superioris – raises the upper eyelid.
- Additionally, there are sympathetic fibres that travel with the superior branch of the oculomotor nerve.
- They innervate the superior tarsal muscle, which acts to keep the eyelid elevated after the levator palpabrae superioris has raised it.
Inferior Branch :
- Inferior rectus – depresses the eyeball
- Medial rectus – adducts the eyeball
- Inferior oblique – elevates, abducts and laterally rotates the eyeball
Parasympathetic Functions :
There are two structures in the eye that receive parasympathetic innervation from the oculomotor nerve:
Sphincter pupillae – constricts the pupil, reducing the amount of light entering the eye.
Ciliary muscles – contracts, causes the lens to become more spherical, and thus more adapted to short range vision.
The pre-ganglionic parasympathetic fibres travel in the inferior branch of the oculomotor nerve. Within the orbit, they branch off and synapse in the ciliary ganglion.
The post-ganglionic fibres are carried to the eye via the short ciliary nerves.
Clinical Relevance:
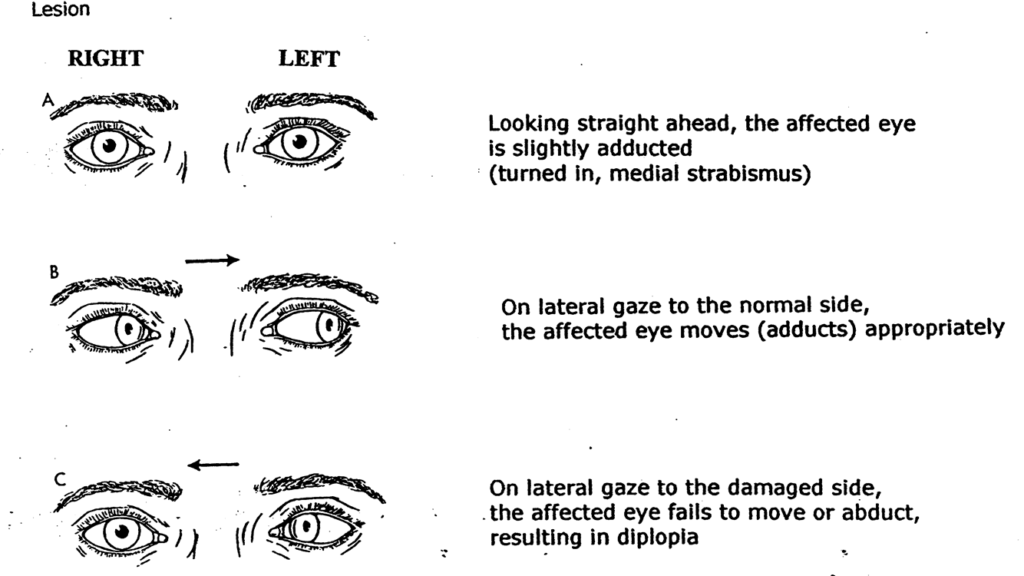
Oculomotor Nerve Palsy :
Oculomotor nerve palsy is a condition resulting from damage to the oculomotor nerve. The most common structural causes include:
- Raised intracranial pressure (compresses the nerve against the temporal bone).
- Posterior communicating artery aneurysm
- Cavernous sinus infection or trauma.
- Note: there are other pathological causes of oculomotor nerve palsy such as diabetes, multiple sclerosis, myasthenia gravis and giant cell arteritis.
The oculomotor nerve provides motor and parasympathetic innervation to some of the structures within the bony orbit.
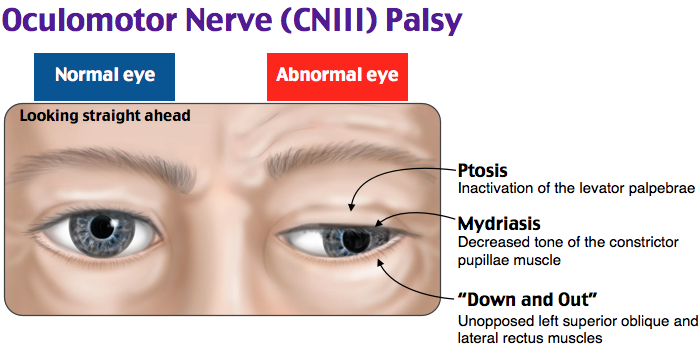
Therefore, the clinical features of CN III injury are associated with the eye:
Ptosis (drooping upper eyelid) – due to paralysis of the levator palpabrae superioris and unopposed activity of the orbicularis oculi muscle.
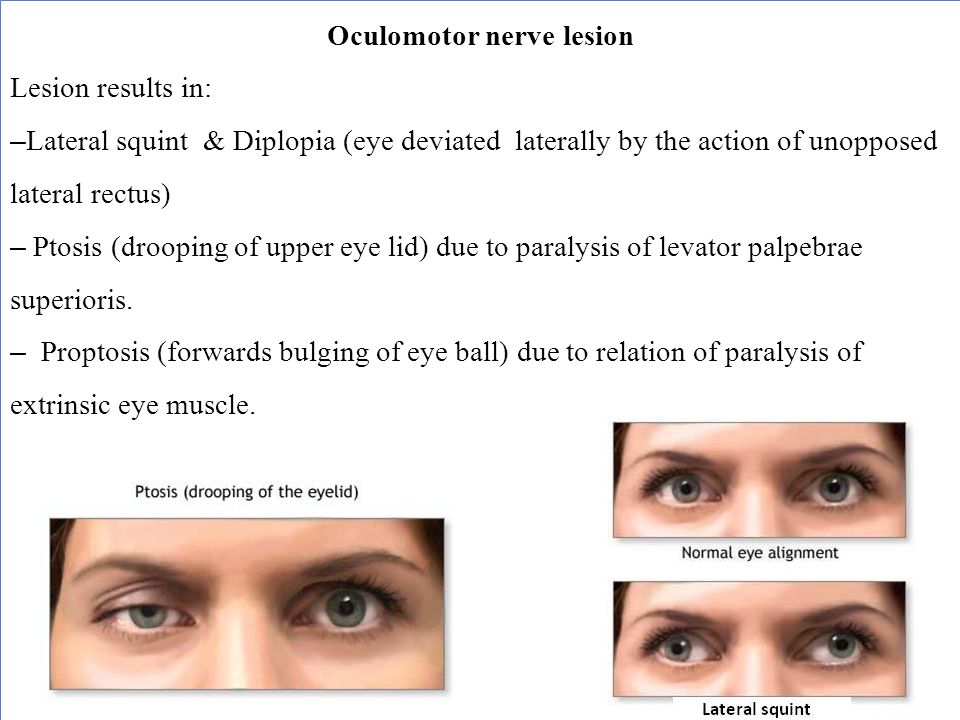
Down and out‘ position of the eye at rest – due to paralysis of the superior, inferior and medial rectus, and the inferior oblique (and therefore the unopposed activity of the lateral rectus and superior oblique).
The patient is unable to elevate, depress or adduct the eye.
Dilated pupil – due to the unopposed action of the dilator pupillae muscle.
Disease :
Paralysis of the oculomotor nerve, i.e., oculomotor nerve palsy, can arise due to:
- Direct trauma
- Demyelinating diseases (e.g., multiple sclerosis)
- Increased intracranial pressure (leading to uncal herniation)due to a space-occupying lesion (e.g., brain cancer) or aspontaneous subarachnoid haemorrhage (e.g., berry aneurysm), andmicrovascular disease, e.g., diabetes.
- In people with diabetes and older than 50 years of age, an oculomotor nerve palsy, in the classical sense, occurs with sparing (or preservation) of the pupillary reflex.
- This is thought to arise due the anatomical arrangement of the nerve fibers in the oculomotor nerve; fibers controlling the pupillary function are superficial and spared from ischemic injuries typical of diabetes.
- On the converse, an aneurysm which leads to compression of the oculomotor nerve affects the superficial fibers and manifests as a third nerve palsy with loss of the pupillary reflex (in fact, this third nerve finding is considered to represent an aneurysm—until proven otherwise—and should be investigated).
other related posts :





9 Comments