

Posterior Tibial Tendon Dysfunction and Physiotherapy tratment
- Posterior tibial tendon dysfunction insufficiency is the most common cause of adult-acquired flatfoot deformity. Failure of the tendon affects surrounding ligamentous structures and will eventually lead to bony involvement and deformity.
- Posterior tibial tendon dysfunction is a progressive and debilitating disorder, which can be detrimental to patients due to limitations in mobility, significant pain, and weakness.
- Tendon degeneration begins far before clinical disease is apparent. Early detection of Posterior tibial tendon dysfunction may prevent operative means of repair; if left to progress, surgical reconstruction with osteotomy and arthrodesis becomes necessary.
- Risk factors for the disease include hypertension, obesity, diabetes, previous trauma, or steroid exposure.
- Posterior tibial tendon dysfunction (PTTD) is a progressive condition that can be classified into four stages.
- In the early stages, there may be pain, the area may be red, warm, and swollen. There are not usually symptoms during gait but symptoms may be present in running.
- Later as the arch begins to flatten, there may still be pain on the inside of the foot and ankle but at this point, the foot and toes begin to turn outward and the ankle rolls inward.
- As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Anatomy related
Posterior tibial tendon dysfunction
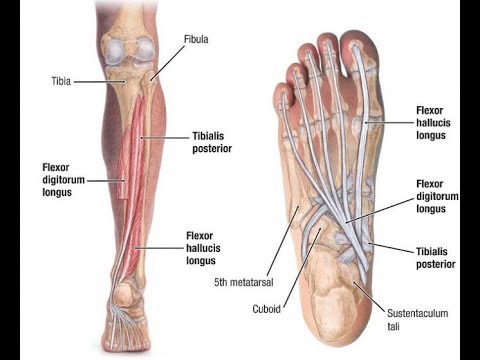
- Tibialis posterior originates from the posterolateral tibia, posteromedial fibula, and interosseous membrane.
- It runs through the deep posterior compartment of the leg and its tendon passes behind the medial malleolus.
- Blood supply to the tendon is the poorest in this area and is the most common site for rupture.
- Close to its insertion site, the tendon splits into a main, plantar and recurrent components, with the main component inserting onto the navicular tuberosity, the plantar portion onto the second, third, and fourth metatarsals, second and third cuneiforms and cuboid. The recurrent component attaches to the sustentaculum tali of the calcaneus.
- Tibialis posterior acts as the primary dynamic stabilizer of the medial longitudinal arch and the main inverter of the midfoot.
- Its contraction also elevates the medial longitudinal arch, causing the hindfoot and midfoot to become a rigid structure. This allows the gastrocnemius to act with greater efficiency during the gait cycle.
- If compromised, a resulting pes planus foot may develop and place greater stress on the surrounding ligaments and soft tissue.
Causes of
Posterior tibial tendon dysfunction
- The most common cause for PTT degeneration is credited to repetitive loading causing microtrauma and progressive failure.
- A retromalleolar, hypovascular region does exist and may also contribute to the disease.
- The anatomic course of the posterior tibial tendon also likely contributes as the tendon does make an acute turn around the medial malleolus, putting a significant amount of tension on the tendon in the region distal and posterior to the medial malleolus (the adjacent tendons of the flexor hallucis longus and the flexor digitorum longus, do not take this sharp turn).
- Other proposed causes are – constriction beneath the flexor retinaculum, abnormal anatomy of the talus, degenerative changes associated with osteoarthritis, and preexisting pes planus.
Symptoms of
Posterior tibial tendon dysfunction
- Most patients report a slow, insidious onset of unilateral flatfoot deformity.
- A history of trauma may be present in up to 50% of cases.
- Patients will describe the pain and swelling along the medial aspect of the foot and ankle, which may be exacerbated with activity.
- Standing on their toes may be painful and difficult, as may walk up or down stairs or on uneven surfaces.
- patients may complain of an exacerbation of a preexisting limp.
- As the medial longitudinal arch collapses, the deformity of the foot increases; in this instance patients may describe abnormal wear on their shoes
Gait in posterior tibial tendon dysfunction
- The functions of a healthy tendon are plantar flexion of the ankle, inversion of the foot, and elevating of the medial longitudinal arch of the foot (it appears as the primary stabilizer of this arch).
- This elevating of the medial longitudinal arch causes a locked entire of the mid-tarsal bones, so the midfoot and hindfoot are stiff.
- This allows the muscle gastrocnemius to act more efficiently during gait.
- With PTTD the other joint capsules and ligaments become weak. The subtalar joint everts, foot abducts (talonavicular joint), and heel is in the valgus position.
- A flattened arch develops what can cause an adult-acquired flatfoot.
- Gastrocnemius is unable to act without the posterior tibial tendon which results in affected balance and gait.
- In below figure, shows different intramuscular EMG activity in tibial posterior activation during walking between acute stage II PTTD to unaffected people.
Differences in muscle activation:
- Participants with PTTD show a significantly greater tibialis posterior EMG amplitude during the second half of the stance phase.
- They walk with a pronated foot and exhibit an increased tibialis posterior activity compared to the participants without PTTD
- In severe cases of deformity, the distal fibula will come into contact with the calcaneus, and pain will move to the lateral aspect of the foot; patients at this stage may describe the feeling of walking on the medial ankle.
- Change in static/dynamic foot ( pes planus)
- Impaired balance
- Impaired MMT PF/IV
- Difficulty/inability to perform unilateral heel raise. Limited calcaneal inversion upon ascent
- Impaired subtalar mobility
Stages of Posterior Tibial Tendon Dysfunction
Stage I: Posterior tibial tendon intact and inflamed, no deformity, mild swelling
Stage II: Posterior tibial tendon dysfunctional, acquired pes planus but passively correctable, commonly unable to perform a heel raise
Stage III: Degenerative changes in the subtalar joint and the deformity is fixed
Stage IV ( Myerson): Valgus tilt of talus leading to lateral tibiotalar degeneration
Stage I
- Deformity: tenosynovitis
- Physical exam: single-leg toe raise test (+)
- Radiography: normal
Stage IIA
- Deformity: Flatfoot deformity, flexible hindfoot, normal forefoot
- Physical exam: single-leg heel raise (-), mild sinus tarsi pain
- Radiography: arch collapse deformity
Stage IIB
- Deformity: Flatfoot deformity, flexible hindfoot/rearfoot, forefoot abduction
- Physical exam: Same stage IIA
- Radiography: same stage IIA
Stage III
- Deformity in stage II becomes fixed, rigid, or inflexible
- Deformity: flatfoot deformity, rigid forefoot abduction, rigid hindfoot/rearfoot valgus
- Physical exam: severee sinus tarsi pain, single-leg heel raise test (-)
- Radiography: arch collapse deformity (subtalar arthritis)
Stage IV
- Deformity: flatfoot deformity, rigid forefoot abduction, rigid hindfoot/rearfoot valgus, deltoid ligament compromise
- Physical exam: single-leg heel raise test (-), severe sinus tarsi pain, ankle pain
- Radiography, arch collapse deformity, subtalar arthritis, talar tilt ankle mortise
Diagnosis of Posterior Tibial Tendon Dysfunction
Examination
- The diagnosis of posterior tibial tendon dysfunction can be made clinically based on history and objective testing.
Subjective
- Before a clinical examination is performed, the patient should be asked a series of questions to rule out other disorders.
- It is essential to diagnose posterior tibial tendon dysfunction (PTTD) in an early phase to prevent permanent deformities of the foot/ankle, a physical examination is therefore essential.
Objective
- The physiotherapist can palpate the posterior tibial tendon from above the medial malleolus to its insertion, to control the integrity and assess possible pain and swelling that are common for the first stages of PTTD.
- In the later stages, the deformity can progress and pes planus may be visible. It is important to examine the whole lower body and not just the foot, as the valgus in the knees can accentuate the appearance of the pes planus.
- A healthy person has a 5° valgus in his hindfoot, in patients with PTTD the valgus is increased and the abduction in the forefoot is also more pronounced The physiotherapist can determine the severity of the pes planus by checking how many fingers can be passed underneath the midfoot.
Special tests for PTTD/AAFD include:
- The too many toes sign: the foot should be inspected from behind and above. The too many toes sign is a manner of inspection from behind.
- in this manner, they can establish if there is an abduction of the forefoot and a valgus angulation of the hindfoot.
- It is based on how many toes you can see from behind. By an affected foot, it will be more than one and a half to two toes see also Foot Posture Index
- Double leg heel rise: to go with both feet from a flatfoot stance to standing on the toes. Patients with stage I dysfunction can do this, but it’s painful.
- Patients with stage II, III, or IV dysfunction are unable to do a heel raise.
- When a patient stands on tiptoes the heel of the affected foot will not bend inwards; the normal foot will stay into inversion while the affected hindfoot will stay in valgus.
- A single-leg heel raise: patients can’t do a single heel raise with the affected foot; The first metatarsal rise sign: the patient stands on both feet, and the shin of the affected foot is taken with a hand and rotated externally.
- When the patient has PTTD, the head of the metatarsal is lifted, while normal metatarsal I stays on the ground; Plantarflexion and inversion of the foot against resistance: to test the power of the tibialis posterior.
Treatment of Posterior tibial tendon dysfunction
- Treatment for posterior tibial tendon dysfunction is a complicated subject, to decide whether patients need operative or non-operative treatment, different variables have to be taken into account by the attending physician.
- Non-invasive therapy, such as orthosis and physical therapy are preferable for they do not damage healthy surrounding tissue, but only when non-operative treatment fails, surgical treatment is required.
- Clear evidence exists that suggests that the quality of life for patients with posterior tibial tendon dysfunction is significantly affected.
- Evidence suggests that early conservative intervention can significantly improve the quality of life regarding disability, function, and pain.
- Treatment for posterior tibial tendon dysfunction is a complicated subject, to decide whether patients need operative or non-operative treatment, different variables have to be taken into account by the attending physician.
All Stages initially:
- Conservative management with NSAIDs and activity modification. Also meant for non-surgical candidates or low-demand, elderly patients.
Stage 1:
- Conservative management through immobilization in a walking boot or cast for up to 3 to 4 weeks to allow for healing of the posterior tibial tendon followed by eccentric strengthening with physical therapy.
- If immobilization and physical therapy are successful, transitioning into custom-molded orthotics or AFO is appropriate to maintain relief. Emphasis on medial forefoot posting is critical.
- Conservative therapy should be for 3 to 4 months, and if it fails, then surgical intervention may be warranted. A tenosynovectomy, with tubularization, may be indicated
Stage 2A:
- Conservative immobilization and physical therapy with orthotics or ankle-foot orthosis (AFO) as recommended in stage 1
- Surgical treatment involves medial calcaneal osteotomy with posterior tendon debridement and repair. Ancillary procedures may include any/all of the following: flexor digitorum tendon (FDL) transfer, spring ligament reconstruction, or Achilles tendon lengthening.
Stage 2B:
- All of the previously listed procedures in Stage 2A +/- lateral column lengthening, or isolated subtalar joint arthrodesis
Stage 3:
- Conservative therapies, as mentioned above.
- Surgical treatment is often warranted as it involves rearfoot arthritic changes and a medial double arthrodesis or triple arthrodesis common (subtalar, calcaneocuboid, and talonavicular arthrodesis) is indicated with or without deltoid ligament repair.
Stage 4
- Conservative therapies, as mentioned above.
- Surgical treatment is often necessary as it involves arthritic changes in the ankle, as well as rearfoot.
- Tibiotalocalcaneal (TTC) arthrodesis for rigid hindfoot with the significant valgus alignment of the talus within the ankle mortise.
Physiotherapy Treatment of Posterior tibial tendon dysfunction
- The key to a successful outcome is early detection of the dysfunction and conservative management to prevent chronicity.
The goals of nonoperative treatment include the
- Elimination of clinical symptoms
- Improvement of hindfoot alignment, and the
- Prevention of progressive foot deformity.
- Patient education reeducation: Activity restriction and modification
- Providing relief through prescriptions for medial arch support insoles or custom orthotics (necessary in many cases).
- Conservative management with physiotherapy and orthotics for Stage I and II is the first option. Options include:
Orthotic devices or bracing: to support the arch.
- A walking cast or CAM boot can be used to immobilize the foot. If this brings relief, the patient can have shoe inserts or modifications, orthotics, or an ankle-foot orthosis (AFO) fitted.
- Achilles tendon stretching and tibialis posterior strengthening, concentric/eccentric training of the posterior tibialis. along with nonsteroidal anti-inflammatories.
- Immobilization: a short-leg cast or boot, that allows the tendon to heal, or avoid all weight-bearing.
- Medications: non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation.
- Shoe modifications: advise changes such as special inserts designed to improve arch support.

- Toe Pick-Ups: The exercise consists of picking up small objects such as pebbles, marbles, or tiny toys with your toes and depositing them in a bucket or other container.
- Arch Strengthening Caterpillar: the arch strengthening caterpillar exercise begins by lying on your back with your knees bent and your feet flat on the floor about two feet from your butt.
- Lift both foot arches and pull your toes back toward your heels. Relax your arches and slide your feet slightly back toward your butt. Repeat the process, allowing your feet to inch closer and closer to your glutes in a caterpillar motion.
- Once your feet are nearly touching your butt, repeat the sequence in reverse, slowly moving your feet away from your butt in the same caterpillar motion.

- Arch Raises: Sit in a chair with your back straight, your knees bent in a 90-degree angle and your feet flat on the floor.
- Raise the arch of one foot off the floor without curling your toes or lifting your heel.
- (It’s much harder than it sounds!) When done properly, you should feel muscle strain in your foot, lower leg, and thigh.
- Alphabet Writing: You can strengthen your entire foot by imagining a pencil in between your toes, pointing the toes outward, and “writing” the alphabet in the air in front of you.
- Up to 4 months of nonoperative treatment should be trialed; if there is no improvement after this period, a tendon synovectomy or debridement may be indicated.




4 Comments