

Retrocalcaneal Bursitis and Physiotherapy Management
- Retrocalcaneal bursitis is the most common heel bursitis. Bursitis is the inflammation of a bursa.
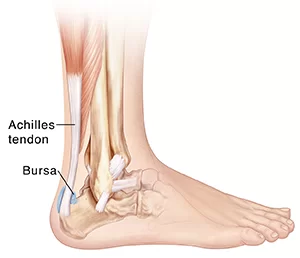
- Retrocalcaneal bursitis is in inflammation of the bursa located between the calcaneus and the anterior surface of the Achilles tendon.
- There are two bursae located just superior to the insertion of the Achilles (calcaneal) tendon.
- Anterior or deep to the tendon is the retrocalcaneal bursa, which is located between the
- Achilles tendon and the calcaneus. Posterior or superficial to the Achilles tendon is the subcutaneous calcaneal bursa, also called the Achilles bursa.
- This bursa is located between the skin and posterior aspect of the distal Achilles tendon. Inflammation of either or both of these bursae can cause pain at the posterior heel and ankle region.
- It is also known as Achilles tendon bursitis. It can often be mistaken for Achilles Tendinopathy or can also occur in conjunction with Achilles tendinopathy.
- A Bursa appears at a junction of a tendon on the bone. A bursa is filled with a thin layer of synovial fluid. It protects and brakes the shocks of the joint.
- The structures nearby the bursa can move with minimal friction due to irritation. The retrocalcaneal bursa is saddled over the posterior-superior prominence of the calcaneus under the Achilles tendon and its lateral expansions.
- The Achilles tendon insertion, the fibrocartilaginous walls of the retrocalcaneal bursae that extends into the tendon, and the adjacent calcaneum form an “ENTHESIS ORGAN”.
- The key concept is that at this site the tendon insertion, the bursa, and the bone are so intimately related that prominence of the calcaneum will greatly predispose to mechanical irritation of the bursa and the tendon. Also, there is a significant strain on the tendon insertion on the posterior aspect of the tendon with dorsiflexion.
Epidemiology of Retrocalcaneal bursitis
- Retrocalcaneal bursitis is common in both the sporting athlete and the general population.
- In the normal population, its incidence is high in individuals who are accustomed to wearing high-heeled shoes on a long-term basis and may experience increased stretch and irritation of the Achilles tendon and its associated bursae when switching to flat shoes.
Causes of Retrocalcaneal bursitis
- A retrocalcaneal bursa mat occurs traumatically from a fall or a sport-related impact contusion or it can also present as a gradual onset due to repetitive trauma to the bursa from activities including running or excessive loading.
- Overtraining in an athleteTight or poorly fitting shoes that produce excessive pressure at the posterior heelHaglund deformityAltered joint axisInflammation of the calcaneal bursae is most commonly caused by repetitive (cumulative) trauma or overuse, and the condition is aggravated by pressure, such as when athletes wear tight-fitting shoes.
- Retrocalcaneal bursitis may also be associated with conditions such as gout, rheumatoid arthritis, and seronegative spondyloarthropathies.
- In some cases, retrocalcaneal bursitis may be caused by bursal impingement between the Achilles tendon and an excessively prominent posterosuperior aspect of the calcaneus (Haglund deformity). In Haglund disease, impingement occurs during ankle dorsiflexion.
Signs and Symptoms of Retrocalcaneal bursitis
- Pain at the back of the heel, especially when running uphill
- Pain may get worse when rising on the toes (standing on tiptoes)
- Tenderness at the back of the heel
- Swelling at the back of the heel
- Increase in pain in activities that load the calf
Assessment
- Good clinical practice includes evaluation of the tendon, bursa, and calcaneum by, careful history,
- inspection of the region for bony prominence and local swelling as well as palpation of the area of maximal tenderness.
- Biomechanical abnormalities, joint stiffness, and proximal soft tissue tightening can exacerbate an anatomical predisposition to retrocalcaneal bursitis, they warrant correction when present.
- Plain radiographs of the calcaneus may reveal a Haglund deformity (increased prominence of the posterosuperior aspect of the calcaneus). However, on weight-bearing lateral radiographs, the
- retrocalcaneal recess often appears normal even in patients with retrocalcaneal bursitis, limiting its
- Usefulness in making this diagnosis. Radiographs may be used as a diagnostic measure to support a clinician’s diagnosis of retrocalcaneal bursitis.
- Individuals with retrocalcaneal bursitis may have an absence of the normal radiolucency (ie, blunting) that is seen in the posteroinferior corner of the Kager fat pad, known as the retrocalcaneal recess or bursal wedge. This may occur with or without an associated erosion of the calcaneus.
- Magnetic resonance imaging (MRI) may demonstrate bursal inflammation, but this modality probably does not offer much more information than that found by careful physical examination.
- Theoretically, MRI could help the physician to determine whether the inflammation is within the subcutaneous bursa, the subtendinous bursa, or even within the tendon itself; however, such testing is generally not necessary.
- Ultrasonography may be a potentially useful tool for diagnosing pathologies of the Achilles tendon.
Differential Diagnosis
- Posterior ankle impingement
- Haglund deformity
- Achilles tendonitis
- partial ruptured Achilles tendon
- Plantar fasciitis
Treatment of Retrocalcaneal bursitis
Physiotherapy Management
The patient with retrocalcaneal bursitis should be instructed to apply ice to the posterior heel and ankle in the acute period of bursitis. Icing can be performed several times a day, for 15-20 minutes each.
- TENS: transcutaneous electrical nerve stimulation is an electrical modality that provides pain relief by providing pain modulation.TENS closes the gate mechanism at the anterior grey horn in the spinal cord. also stimulates the endogenous opioid system which prevents the release of substance p at the anterior grey horn.
- IFT: Interferential current therapy produces a low-frequency effect at targeted tissue, it inhibits transmission of pain impulses, stimulates the endogenous opioid system, increases blood supply, relieves edema, and removes the waste products.
- contrast bath therapy: Contrast bath therapy, is a form of treatment where a limb or the entire body is
- immersed in hot (but not boiling) water followed by the immediate immersion of the limb or body in cold ice water. This procedure is repeated several times, alternating hot and cold. It relieves inflammation of bursae, swelling and reduce pain
Ankle joint Range of motion exercise
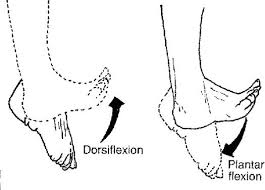
- dorsiflexion
- plantarflexion
- eversion
- inversion
Gradual progressive stretching of the Achilles tendon may help relieve impingement on the subtendinous bursa and can be performed in the following manner:
- Stand in front of a wall, with the affected foot flat on the floor. Lean forward toward the wall until a gentle stretching is felt within the ipsilateral Achilles tendon.
- Maintain the stretch for 20-60 seconds and then relax. Perform the stretches with the knee extended and then again with the knee flexed.
- To maximize the benefit of the stretching program, repeat the above steps for several stretches per set, several times daily. Avoid ballistically (ie, abrupt, jerking) stretches.
- Other treatment options are microcurrent therapy and corticosteroid injection into the retrocalcaneal bursa
Strengthening exercise:
- Start by sitting with your foot flat on the floor and pushing it outward against an immovable object such as
- a wall or heavy furniture. Hold for about 6 seconds, then relax. After you feel comfortable with this, try using rubber tubing looped around the outside of your feet for resistance.
- Push your foot out to the side against the tubing, then count to 10 as you slowly bring your foot back to the middle. While still sitting, put your feet together flat on the floor. Press your injured foot inward against your other
- foot. Hold for about 6 seconds, then relax. Next, place the heel of your other foot on top of the injured one. Push down with the top heel while trying to push up with your injured foot. Hold for about 6 seconds, then relax.
Weight-bearing exercise

- walk-on toe
- walk-on heel
- toe standing
- heel standing
Balance exercise:

- Stand on just your injured foot while holding your arms out to your sides with your eyes open.
- If you feel unsteady, stand in a doorway so you can put your hands on the door frame to help you.
- Balance for as long as you can, working up to 60 seconds. When you can do this for 60 seconds. Stand on your injured foot only and hold your arms across your chest with your eyes open.
- When you can do this for 60 seconds. Stand on your injured foot only, hold your arms out to the sides, and close your eyes. If you feel unsteady, stand in a doorway so you can put your hands on the door frame to help you.
- When you can do this for 60 seconds, try exercise number. Stand on your injured foot only, hold your arms across your chest, and close your eyes. Balance for a long as you can, working up to 60 seconds.
Proprioceptive training:
- proprioceptive training on bosu
- proprioceptive training on wobble board
- proprioceptive training in the balance board
Surgical
- Whilst rare, un-resolving cases of retrocalcaneal bursitis may result in a bursectomy where the bursae are removed from the back of the ankle.

Author: Bhoomi Physiotherapist
Bhoomi Patel - Physiotherapist in Mobile Physiotheray Clinic, B - 01, Jagatnagar Society, Opp. Shaktidhara Society, India Colony Road, Tollnaka, Bapunagar, Ahmedabad.



2 Comments