

Scapulocostal Syndrome
Introduction
Scapulocostal syndrome is a musculoskeletal condition characterized by pain and dysfunction in the region where the scapula (shoulder blade) and the ribs meet. This syndrome is often associated with discomfort or pain in the upper back, specifically in the area where the scapula attaches to the thoracic (rib) cage.
It is also called snapping scapula syndrome or scapulothoracic syndrome. This condition is caused by a disruption in the usual scapulothoracic mechanics.
The scapulocostal syndrome is an overuse condition produced by repeated incorrect usage of the levator scapulae, pectoralis minor, serratus anterior, rhomboids, and, to a lesser extent, infraspinatus and teres minor muscles of scapular stabilization. It is a persistent myofascial pain syndrome, and the discovery of myofascial trigger points on physical examination is the sine qua non of myofascial pain syndrome.
Symptoms include unilateral discomfort and accompanying paresthesias along the scapula’s medial border, referred pain radiating from the deltoid area to the dorsum of the hand, and limited scapula range of motion. The majority of instances are observed in young, vigorous patients who overuse the overhead or throwing motion. The scapulocostal syndrome is also known as a traveling salesman’s shoulder because it is typically found in people who stretch backward to collect something from the rear seat of an automobile.
Doctors frequently give anti-inflammatory drugs as well as physical treatment to strengthen the subscapularis muscle. Cortisone injections would be used in severe situations.
What is the Scapulocostal Syndrome?
Snapping scapula syndrome can be defined as an audible or palpable snapping, grinding, or crepitus sounds of the scapula during scapulothoracic joint motions. It is more of a symptom of another condition. It is most frequent in young, energetic people.
Individuals with this condition frequently have a history of pain, stiffness, and weakness with overhead motions, which can be caused by sports or overuse. The symptoms of snapping scapula syndrome might be mild and are caused by trauma or excessive grinding of the scapula and thorax with soft tissues entrapped between them, such as bursas, muscles, or tendons.
Isometric motions do not usually reproduce pain. The clicking and popping, as well as the discomfort, generally decrease when the arm is crossed across the chest, causing the scapula to rise off the rib cage. This condition is frequently ignored because of a lack of knowledge regarding the diagnosis.
What areas of the body are affected by this condition?
The humerus (upper arm bone), clavicle (collarbone), and scapula (shoulder blade) are the three bones that make up the shoulder. Two big muscles attach to the scapula’s front half, which lies against the chest wall. The subscapularis muscle joins to the front of the scapula where it confronts the chest wall. The serratus anterior muscle joins to the scapula closest to the spine. It runs in front of the scapula, loops around the chest wall, and attaches to the front ribs.
A bursa is a fluid-filled sac that acts as a cushion between bodily tissues. A bursa is located between the scapula’s two muscles. A bursa can also be seen between the serratus anterior muscle and the chest wall. Bursitis is a disorder that occurs when the bursa sacs become inflamed.
Scapulothoracic bursitis is defined as inflammation of the bursa beneath the shoulder blade. This form of bursitis is more frequent in the upper scapular corner closest to the spine. It can also be found beneath the lower point of the scapula. It can create the sounds and symptoms of snapping scapula syndrome in any situation. Bursitis in the joint can occur without any grinding or popping.
Cause of the Scapulocostal Syndrome
When the muscles beneath the scapula (the subscapularis muscle) atrophies, this can cause a snapping scapula. As a result, the scapula becomes extremely near to the rib cage, resulting in rubbing or bumping during arm/shoulder movement. Bursitis is another cause, which occurs when the tissues between the shoulder blade and the thoracic wall become inflamed. Shoulder muscle and bone problems can also lead to discomfort.
Repetitive actions that create inflammation or atrophy of the muscles beneath the scapula can cause this illness. A fracture that affects the form of the scapula, or an injury to the ribcage that leads to a rib protruding out from its natural position, can also cause it.
Symptoms of the Scapulocostal Syndrome
Snapping Scapula Syndrome develops in a variety of ways that might interfere with an individual’s daily activities and overall shoulder function. These manifestations, which are frequently caused by an unusual interaction of the scapula with the rib cage, can vary from auditory complaints to discomfort and abnormal movement patterns. Here are some of the important features and manifestations of this condition:
- Patients frequently describe popping, clicking, and grinding as auditory or tactile feedback symptoms during overhead arm motions. It is caused by the scapula rubbing on the ribs or the thoracic spine.
- Pain with Overhead Movements: Activities that require elevating the arm, such as reaching for an object on a high shelf or executing sports moves, might cause discomfort.
- Pain Presentation: The nature of the pain might vary. Depending on the individual and the underlying causes, it might be dull and chronic, a continual ache, or even acute, abrupt jabs. gradual onset of pain in the superior or posterior aspect of the shoulder girdle, with radiating pain into one or more of the following areas
- The neck and occiput, which is frequently associated with severe headache
- The upper arm, specifically in the upper triceps and insertion point of the deltoid muscle
- Around the chest to the front of the thoracic wall and down the medially.
- Lack of Coordinated motions: This refers to the inability to move the shoulder smoothly and effectively over its whole range of motion, which frequently results in limited mobility or compensatory motions.
- Weakness: Affected people may notice a decrease in strength in their shoulder or upper arm, limiting their ability to perform everyday activities or particular jobs.
- Winging of the Scapula: This is one of the syndrome’s distinguishing features, and it refers to the scapula projecting outwards, away from the thoracic wall. This is sometimes clearly visible.
- Abnormal Scapular Movements: In addition to winging, the scapula may not follow its regular movement pattern, resulting in a variety of additional shoulder disorders.
Examination
If a physical therapist suspects a patient has snapping scapula syndrome, they may ask the following questions throughout the examination process:
- When and how did you first become aware of the pain?
- What activities cause you to hear or feel popping, clicking, and grinding?
- Do you experience any neck discomfort or stiffness?
- Is your shoulder weak or “tired?”
Special Examinations
There are no particular tests for snapping scapula syndrome; however, there are tests to rule out other scapula diseases.
Scapular Assisted Test:
- The patient will stretch his or her shoulders forward.
- The physical therapist can assist the patient during forward shoulder flexion by fostering appropriate scapular mechanics by stabilizing the upper scapular border and assisting with inferomedial border upward rotation.
- The unsupported movement will be compared to the assisted movement by the physical therapist.
- This is a positive (+) test if the patient feels better after receiving support.
Scapular Lateral Slide Test
- The patient is instructed to abduct the affected arm to 0, 45 (with internal rotation), then 90 (with maximum internal rotation).
- The physical therapist measures the distance between the inferior angle of the scapula and the thoracic spinous process at the same position.
- In comparison, the physical therapist performs steps one and two on the non-involved side.
- A positive (+) test is indicated when a side-to-side difference of 1-1.5 cm is measured.
Diagnosis
X-ray: X-ray to view the area between the rib cage and scapula. An X-ray picture can reveal bone abnormalities such as a scapular or rib fracture.
CT scan: When a doctor suspects a bone condition, a computed tomography (CT) scan may be ordered to provide a more thorough examination.
Magnetic resonance imaging (MRI): MRI may be used to find the bursa and measure its size if bursitis is suspected. Magnetic waves are used in MRI scans to display the body’s soft tissues in slices.
Electromyography (EMG): Electromyography (EMG) is a diagnostic technique that gauges nerve and muscle electrical activity. It can assist in identifying any nerve injury or malfunction as well as determining whether the muscles are working properly.
Nerve Conduction Study (NCS): This diagnostic test measures the strength and speed of nerve signals, much like an EMG does. It can assist in identifying any nerve impairment or dysfunction that might be causing the discomfort.
Ultrasound: Ultrasound creates images of the muscles and soft tissues by using high-frequency sound waves. It can assist in identifying any soft tissue tears, edema, or inflammation in the muscles.
Treatment of Scapulocostal Syndrome
The Conservative treatments available may include rest, ice, anti-inflammatory medicines, cortisone injections, and physical therapy. If such therapies fail, surgery to modify the form of the scapula may be required.
Conservative treatment
Surgical intervention is usually not necessary when scapulothoracic popping and clicking is associated with a soft tissue defect, poor posture, or scapular dyskinesis.
The Conservative treatments may include
- Rest and ICE.
- NSAIDs,(non-steroidal anti-inflammatory drugs)
- a cortisone injection, usually three to four times a year, into the area beneath the scapula where the inflammation is present
- Physical therapy
If such therapies fail, surgery to modify the form of the scapula may be required.
The Surgical Treatment
Scapular dissection: Friction between the ribs may cause a conspicuous bony piece of the scapula to be removed.
Bursectomy: The scapulothoracic space’s inflammatory tissue is removed during an arthroscopic scapulothoracic bursectomy.
A scapulothoracic bursectomy involves removing the inflammatory bursa between the ribs and scapula as well as shaving off a portion of the medial angle beneath the scapula. The patient can go home on the same day because this operation is performed as an outpatient procedure. Typically, recovery takes four to six months. The patient will be forced to limit their movement for the first four weeks following the operation by wearing a sling, and in the fifth week, they will begin physical therapy.
Physical therapy management
When it comes to treating Snapping Scapula Syndrome, physical therapy is essential. Physical therapists can treat the underlying dysfunctions that lead to the illness using a variety of modalities, therapeutic exercises, manual treatments, and instruction on posture and movement mechanics.
Patients can benefit from reduced discomfort, better scapular kinematics, and regained shoulder function with customized therapy strategies. The following are some of the main strategies and interventions used in the physical therapy treatment of this syndrome:
- Heat/Ice packs
- Ultrasound
- Heatstroke
- Stimulation using Electrical
- Laser Therapy
- Scapular Soft Tissue Massage
- Releases of Shoulder, Neck, and Chest Trigger Points
- Exercises that strengthen the rotator cuff, rhomboids, mid and lower trapezius, and serratus anterior
- Levator Scapulae, Upper Trapezius, Latissimus Dorsi, Subscapularis, Sternocleidomastoid, Rectus Capitis, and Scalene muscles should all be stretched.
- Take care of the patient’s posture to ensure that the kinetic chain pattern is followed by the patient’s head, neck, and shoulders.
- Kinesiotaping the shoulder blade
- Arm, neck, shoulder, and scapula passive motions
Exercises for Scapulocostal syndrome
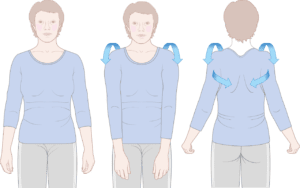
Shoulder rolls
Shoulder rolls are a simple yet effective exercise for improving shoulder mobility, flexibility, and posture. They may be used as a warmup before exercise, a cooldown afterward, or simply to relax your shoulders throughout the day.
Here’s how to perform forward and backward shoulder rolls:
- Maintain proper posture by standing or sitting with your back straight and your shoulders relaxed.
- Allow your arms to hang at your sides naturally.
- Begin circularly rolling your shoulders, forming huge circles with them.
- Begin by moving your shoulders forward, up towards your ears, backward, and down.
- Perform 15-20 forward shoulder rolls.
- Shoulder rolls in the back:
- Repeat the forward shoulder roll movements, but this time roll your shoulders in the other direction.
- Roll your shoulders backward, down towards your spine, and then up and forward.
- Perform 10 to 15 backward shoulder rolls.
- Maintain moderate and controlled motions.
- Make broad circles with your shoulders rather than little shrugs.
- Throughout the activity, breathe properly.
- Stop and see a doctor or physical therapist if you have any pain.
Cat Cow Pose
This basic yet adaptable exercise has several advantages for your spine, core, and general health.
How to perform It:

- Begin on all fours, hands shoulder-width apart and immediately beneath your shoulders. Knees should be hip-width apart and squarely beneath the hips.
- In the Cow Pose Inhale deeply while arching your back upwards, lowering your abdomen, and slightly raising your chin. Consider yourself a happy cow feeding in a farmland. Maintain a long neck and an upward glance.
- In the Cat Pose Exhale deeply, inwardly curving your back, tucked your chin to your chest, and pressing your abdomen into your spine. Consider a happy cat curled up in a ball.
- Repeat the moves multiple times, synchronizing your breath with your movement. Inhale the Cow and expel the Cat.
- Concentrate on creating smooth, controlled motions and paying attention to your body. If you experience any discomfort, stop.
- Maintain a neutral posture and avoid dropping your shoulders down towards your ears.
- Throughout the exercise session, breathe deeply and evenly.
- You may adjust the exercise by sitting on your heels with your hands alongside you, or by performing it on your knees instead of your hands.
Scapular Retraction
Scapular retraction is a critical movement for maintaining good shoulder health and posture. It’s frequently used in a variety of workouts and stretches to increase flexibility, prevent injuries, and even relieve neck and back discomfort.

- Begin by standing or sitting with proper posture. Straighten your back, relax your shoulders, and place your feet level on the floor.
- Consider squeezing your shoulder blades together instead of shrugging your shoulders up towards your ears. Maintain a long neck and a forward stare.
- Hold the retraction for a few seconds before gradually releasing it.
- Repeat 10-15 times more. Prioritise quality above quantity.
- It is more crucial to do the retraction correctly than to perform a great number of repetitions incorrectly.
Scapular Shrug
The scapular lift, often known as the scapular shrug, is a great exercise for strengthening the muscles surrounding your shoulder blades and increasing shoulder mobility.
Here’s how to do it correctly:
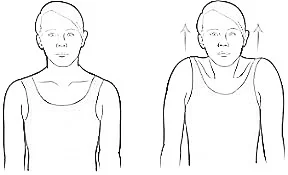
- Begin in a proper posture, either standing or sitting. Maintain a straight back, relaxed shoulders, and flat feet on the floor.
- Lift your shoulder blades slightly upwards towards your spine, as if attempting to touch your shoulder blades together above your head. Don’t tighten your jaw or shrug your shoulders.
- Hold the lift for a few seconds before lowering your shoulder blades to their starting position.
- Do this 10-15 times.
- Concentrate on experiencing movement in your upper back rather than simply your shoulders.
- Throughout the activity, breathe properly.
- Lifting your shoulders too high might strain your neck.
- Stop and get medical attention if you experience any pain.
The Prone “Y”
The prone “Y” exercise is an isometric exercise, which means you retain a static position with no movement.
How to perform It:
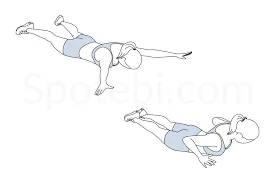
- Begin by laying face down on a mat, legs straight and feet relaxed.
- Position to begin the Prone Y exercise.
- Extend your arms to the sides of your body, producing a “Y” shape. Thumbs should be pointed up towards the ceiling, and arms should be somewhat below shoulder height.
- Squeeze your shoulder blades together and down towards your spine to activate your lower trapezius muscles. Consider pulling your shoulder blades into your back pockets.
- Maintain this position for 10-15 seconds, focusing on proper form and regulated breathing. Do not shrug your shoulders or arch your back.
- Relax your muscles and slowly return your arms to their initial position.
- Repeat the exercise 2-3 times for a total of 10-15 repetitions.
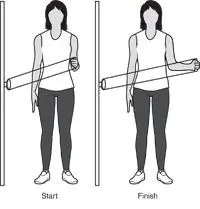
External and internal rotation
External and internal rotation workouts target the rotator cuff muscles, a group of four muscles that assist in stabilizing the shoulder joint. Strengthening these muscles can aid with shoulder stability, pain relief, and injury prevention.
How to Perform an External Rotation with a Theraband
- Attach the theraband to a doorway or other solid item around your waist.
- Place your feet shoulder-width apart and face away from the hook while standing.
- Hold the theraband in your hand, elbow bent at 90 degrees, and arm near to your side.
- Keep your elbow bent and near to your side as you rotate your arm outward.
- Return your arm to the initial stance gradually.
- Do this in three sets of ten to twelve repetitions each.
How to Perform an Internal Rotation with a Theraband

- Attach the theraband to a doorknob or other solid item around your waist.
- Position yourself facing the anchor with your feet approximately shoulder-width apart.
- Hold the theraband in your hand, elbow bent at 90 degrees, and arm near to your side.
- Keep your elbow bent and close to your side as you rotate your arm inward.
- Return your arm to the initial stance gradually.
- Do this in three sets of ten to twelve repetitions each.
Serratus Anterior Punches

The serratus anterior muscle, sometimes known as the “boxer’s muscle,” is essential for shoulder stability and movement.
Serratus Anterior Punches are performed as follows:
- Begin in a high plank posture, with your hands shoulder-width apart, just under your shoulders, and your fingers pointing forward.
- Imagine throwing a punch outwards, pulling your shoulder blades towards your spine, and tightening your serratus anterior muscles. With each blow, concentrate on feeling your shoulder blades “protract” (go forward).
- Keep your spine neutral and your core engaged. Allow your lower back to droop or arch. Keep your core engaged throughout the action to keep your body stable.
- Return to your starting point. Bring your elbows in slowly, maintaining your shoulder blades protracting, until you reach the high position.
- Repeat 10-12 times more: Aim for three sets, progressively increasing the number of reps or sets as you gain strength.
Preventative Actions
It is vital to prevent the recurrence of Snapping Scapula Syndrome. Implementing certain steps can reduce the pressure on the scapulothoracic joint, reducing the risk factors that lead to the start or worsening of the illness.
Consider the following critical preventive measures:
- Maintain an erect posture and avoid drooping.
- Maintain scapular strength as well as the muscles that surround the shoulder joint.
- When executing overhead arm motions, use proper technique.
- Maintain flexibility in the neck, shoulder, and scapular muscles.
FAQs
What exactly is scapulocostal syndrome?
Snapping scapula syndrome is characterized as an audible or palpable snapping of the scapula during scapulothoracic joint motions. It often affects young, energetic individuals who frequently describe a history of discomfort caused by overuse, quick shoulder motions, or sports activities.
Which fascia is affected by Scapulocostal syndrome?
Scapulocostal syndrome (SCS) is a chronic myofascial pain syndrome (MPS) that affects the posterior scapular myofascial components, including the serratus posterior superior, rhomboid minor and major, and levator scapulae muscles, as well as the fascia around these muscles.
What is the cause of scapula syndrome?
In most cases, repeated actions produce inflammation. Certain repetitive shoulder actions, such as pitching baseballs or hanging wallpaper, might promote inflammation of the joint tissues.
What is the location of the Scapulocostal joint?
The scapulothoracic junction connects the scapula’s anterior side to the thoracic wall’s superolateral surface. The former is somewhat concave anteriorly, while the latter is convex as a result.
How is scapula syndrome treated?
Conservative management
Nonsteroidal anti-inflammatory drugs (NSAIDs) Cortisone injection into the area beneath the scapula where inflammation develops; usually repeated 3-4 times per year.
Physiotherapy.
References
- Themes, U. (2019, September 9). Scapulocostal Syndrome. Anesthesia Key. https://aneskey.com/scapulocostal-syndrome/
- Wikipedia contributors. (2022, July 1). Snapping scapula syndrome. Wikipedia. https://en.wikipedia.org/wiki/Snapping_scapula_syndrome
- Scapulocostal Syndrome: Unraveling the mystery of scapular pain – FasterCapital. (n.d.). FasterCapital. https://fastercapital.com/content/Scapulocostal-Syndrome–Unraveling-the-Mystery-of-Scapular-Pain.html
- Russek, A. S. (1952). DIAGNOSIS AND TREATMENT OF SCAPULOCOSTAL SYNDROME. JAMA, 150(1), 25. https://doi.org/10.1001/jama.1952.03680010031007



2 Comments