Superior Thyroid Vein
Introduction
The superior thyroid vein is an important vascular structure within the neck that plays a critical role in venous drainage. It originates from the venous plexus of the thyroid gland and primarily drains blood from the superior part of the thyroid gland and surrounding areas.
The vein ascends obliquely, accompanying the superior thyroid artery, and eventually empties into the internal jugular vein. Its anatomical position and clinical relevance make it significant in thyroid surgeries and neck procedures, as it can be a source of bleeding or serve as a landmark for surgeons. Among all others, this is the largest vein that comes from it and goes into a brachiocephalic vein after emptying its contents at the lower side. The optimal functioning of these vessels is imperative for maintaining healthy thyroids and overall hormonal balance. Thyroid disorders may develop when there are interruptions or anomalies in these veins. To diagnose and treat thyroid-related disorders and during operations involving the thyroid gland, knowledge of the structure and physiology of thyroid veins is necessary.
What is the origin of Superior Thyroid Vein?
The glands inside and around the thyroid gland give rise to the superior thyroid gland. It collects blood from the surface of the thyroid gland, and frequently receives streams from the surrounding tissues, including the upper oral mucosa.
The muscle ascends next to the superior thyroid gland and drains into the internal jugular vein, Typically, it is located at the level of the hyoid bone, and its path and relationship with the thyroid gland and the nervous system significantly impact the nervous system. And also Location: The upper fragment of the thyroid gland is evacuated by the superior thyroid veins.
In the human anatomy, they are typically observed on either side of the thyroid gland and extend upward towards the internal jugular veins in humans. Drainage: They often drain into the internal jugular veins, which are big veins that run in conjunction on both sides of the neck.
What structures does the superior thyroid vein drain?
The superior thyroid vein drains several structures associated with the thyroid region. This includes the following structures:
- Thyroid gland: The main structure that is drained by the superior thyroid vein, encompassing the upper sections of the gland.
- Larynx: Portions of the larynx, particularly structures near its superior aspect.
- Adjacent muscles and tissues: Some drainage may include parts of the surrounding infrahyoid muscles and nearby soft tissues. The superior thyroid gland drains into the internal jugular vein, which returns the gland from the neck to the systemic fluid.
Where does the superior thyroid vein terminate?
The upward-moving thyroid gland typically ends at the internal jugular vein. It collects blood from the thyroid gland, larynx, and close by systems and publications upward to drain into the internal jugular vein, normally near its decrease phase.
How does the superior thyroid vein relate to the thyroid gland anatomically?
Elevated thyroid gland is closely associated anatomically with the thyroid gland. Here are the basic facts about the time of its formation:
- Origin: The superficial gland arises from a vein below the thyroid gland, and usually drains blood from the superior portion of the gland.
- Pathway: It ascends from the thyroid gland and courses laterally and superiorly. The vein typically follows the path of the superior thyroid artery, running alongside it but draining blood rather than supplying it. Drainage: Blood that has lost oxygen is transported from the upper portion of the thyroid gland by the superior thyroid vein. It ultimately drains into the internal jugular vein on each side.
- Anatomical Relations: It is situated close to the upper pole of the thyroid gland. As it ascends, it may cross paths with the external branch of the superior laryngeal nerve, which serves to innervate the cricothyroid muscle. The superior thyroid gland plays a role in the drainage system, which also encompasses the middle thyroid gland and the inferior thyroid gland to enhance blood flow away from the gland.
Are there any differences in the anatomy of the superior thyroid vein?
Superficial thyroid vein (STV) anatomy is common and this can be clinically significant, especially for surgeries or procedures involving the neck. Here are a few surprising changes:
- Number of glands upper STV is usually one gland on each side, but numbers may vary in some individuals Thyroid rather than STV Multiple glands may be present that drain the gland.
- Conclusion Normal conclusion: STV usually drains into the internal jugular vein (IJV). Differential incision: This may flow into the common anterior vein or directly into the greater posterior vein. Rarely, it may terminate in the subclavian vein.
- The form and supporting course of the STV may vary somewhat, especially concerning surrounding structures such as the sternocleidomastoid muscle. Its streams, which typically drain the thyroid gland, larynx, and a portion of the proximal glands, vary in the number, size, or shape of anastomoses.
- Anastomoses STV may be associated with other glands, such as the central thyroid gland, the inferior thyroid vein, or anterior jugular vein, the thyroid vein is composed of surrounding tissues
- Asymmetry Left and right can differ from one another. For example, the size, number, or termination of the STV may differ on the two sides.
Clinical Significance Surgical relevance: Knowledge of these variations is critical during procedures like thyroidectomy or neck dissection to avoid inadvertent injury, which can lead to excessive bleeding or complications. Radiological relevance: Variations in the STV may affect the interpretation of imaging studies such as ultrasonography or CT angiography of the neck.
What is the primary function of the superior thyroid vein?
Superficial blood vessels are blood vessels that primarily function to drain blood from the thyroid gland and nearby structures collect deoxygenated blood from the thyroid gland and surrounding tissues and deliver it to the jugular vein of the inner cavity, and finally return blood to the heart The gland.
- Drainage Location: Drains blood: from above thyroid gland. Adjacent areas such as the larynx and larynx.
- Termination: Usually placed in an internal roller. This gland plays an important role in the vasoconstriction of the thyroid gland and helps maintain proper blood flow in the neck.
How does the superior thyroid vein contribute to nerve flow in the neck?
Superficial fluid is an important fluid in the neck, especially where the thyroid gland is located. Here’s how it contributes:
- Anatomical pathway: The upper thyroid gland arises from the muscles surrounding the upper thyroid gland. It passes up and down, and it passes up to the thyroid gland, although it is not closely connected.
- Drainage: The thyroid drains blood from the apex of the gland and adjacent structures, often receiving streams from parts of the thorax, larynx, and infrahyoid region
- Conclusion: The gland drains into the intraperitoneal vein (IJV). ), usually near or at its origin. This relationship facilitates reperfusion of the circulatory system. Functional Significance: The superior thyroid gland promotes efficient drainage from the thyroid gland and surrounding tissues.
Is there a function for coronary heart fee in thyroid hormone shipping?
The gland itself isn’t an immediate transporter of thyroid hormone, but it performs a function within the widening of the circulatory machine with the aid of appearing as a vasoconstrictor How it works:
- Thyroid hormone secretion: Thyroid gland Thyroid hormone (especially thyroxine [T4] and triiodothyronine [T3]) blood Vessels to the secretory thyroid: Blood from the thyroid gland of the thyroid gland, its secreted hormones are carried into the gland through the way of the advanced, middle, and inferior thyroid glands These glands carry blood from the thyroid gland to the aorta.
- Transport: Once within the bloodstream, thyroid hormones are sure to proteins inclusive of: thyroxine-binding globulin (TBG) and transthyretin (TTR) albumin These proteins transport thyroid hormone at some stage in tissues and nerves, ensuring distribution to tissues for the duration of the body.
- Tissue secretion: After circulating through muscle tissues and tissues, thyroid hormones are launched from their shipping proteins and brought up using epithelial cells, wherein they are fed on by their metabolites function In precis, while tissues (inclusive of arteries) offer the pathway essential for thyroid hormone to flow into in the blood The real transport of cells in the body relies upon on plasma and transport proteins on The frightened gadget is a Circulatory loop that allows for the green shipping of those hormones.
What are the common conditions affecting the superior thyroid vein?
The superior thyroid gland is a vein that drains blood from the thyroid gland and nearby structures to the internal jugular vein Although the gland itself is rarely the primary site of infection, it often can be associated with or affected by thyroid or vascular diseases ( enlarged thyroid): A large goiter, especially if retrosternal, may compress or alter the course of the superior thyroid gland. May affect lymphatic drainage.
- Thyroid gland or bladder: Malignant or large benign glands may become lodged or compressed.
- Thyroiditis (Inflammation): Hashimoto’s thyroiditis: Chronic inflammation can cause congestion in the localized glands.
- De Quervain’s thyroiditis: Severe inflammation may sometimes be accompanied by the formation of glands.
- Hyperthyroid or hypothyroid: This conditions may cause muscle spasms in conditions including hyperthyroidism (thyroid inferno) Graves disease, in which all three apical thyroid glands may be abnormal Surgery or headache.
- Intervention Thyroidectomy or parathyroidectomy: Thyroid is often elevated in these pathways in Happened knots can occur Tied up or untreated, with injury or obstruction of the muscle in can cause complications including bleeding due to poor blood flow. Central line placement or neck surgical treatment: Procedures regarding the internal jugular vein can also inadvertently affect the superior thyroid vein.
- Muscle harm Local vasculitis: Rare, however, can also occur throughout surgical procedures, trauma, or immoderate coagulation. Internal jugular vein thrombosis: Secondarily, the superficial thyroid vein, and different vessels can be involved.
- Compression by using way of manner of Neck Masses Enlarged lymph nodes, cysts, or distinctive tumors in the neck can compress the advanced thyroid vein, number one to venous engorgement or altered drainage patterns.
- Congenital or Vascular Anomalies Anatomical variations within the advanced thyroid vein or its tributaries can also additionally predispose individuals to headaches in the course of scientific or surgical interventions.
- Infectious or Inflammatory Processes Lemierre’s Syndrome: A rare situation related to thrombophlebitis of the inner jugular vein secondary to oropharyngeal infection may additionally amplify to tributaries just like the advanced thyroid vein.
- Increased Intrathoracic Pressure Conditions like advanced vena cava (SVC) syndrome or good-sized thoracic masses can lead to venous congestion within the neck, involving the superior thyroid vein. Clinical Implications Symptoms related to superior thyroid vein situations are regularly subtle and overshadow the useful resource of the primary pathology (e.g., thyroid swelling, neck ache, or venous congestion). Doppler ultrasonography is typically used to assess venous go-with-the-flow in thyroid and neck pathologies.
Proper identity and coping with the superior thyroid vein are important in the course of surgical strategies to prevent headaches. If a selected situation is suspected, further investigations and management might be tailor-made accordingly.
How is the superior thyroid vein involved in thyroidectomy or neck surgeries?
The ascending thyroid gland is an important anatomic concern in thyroidectomy or neck surgery, especially because of its proximity to the thyroid gland and its properties when acting here:
- Anatomy: The elevated thyroid gland drains the upper thyroid gland. It commonly empties into the internal jugular vein or the brachiocephalic vein. This vein runs alongside the advanced thyroid artery and is situated close to different essential systems like the recurrent laryngeal nerve.
- Role in Thyroidectomy: During a thyroidectomy, that is the surgical removal of all or a part of the thyroid gland, the medical professional needs to carefully manipulate and ligate (tie off) the advanced thyroid vein to control bleeding and make sure proper surgical entry to to the gland. The vein’s proximity to different vital systems just like the recurrent laryngeal nerve and parathyroid glands requires careful dissection to avoid harm.
- Bleeding Control: The advanced thyroid vein is exceptionally small in evaluation to arteries, however, it nonetheless carries a widespread quantity of blood from the thyroid gland. Surgeons regularly use electrocautery or ligation techniques to control venous bleeding from the vein during the dissection of the thyroid gland. Any failure to govern bleeding from the vein can cause postoperative complications, such as hematomas.
- Anatomical Variations: Surgeons should be aware of capability variations in the anatomy of the superior thyroid vein. It can also have two streams, be on either side of the thyroid gland, or have an abnormal orientation. Knowing those definitions makes it easier to prevent damage or unintentional bleeding.
In summary, the superior thyroid gland is an important structure that must be carefully managed during thyroid and neck surgery to avoid complications such as bleeding and to ensure close hits as protection of the nerves and parathyroid glands.
What are the potential complications of injuring the superior thyroid vein during surgery?
Injuries to the superficial thyroid gland at some point during surgery can cause many possible complications depending on volume loss, and associated environmental factors Here are a few potential complications:
- Haemorrhage: Injury to the superficial thyroid gland is the main artery for thyroid bleeding due to which various vital structures in the neck Due to proximity, when bleeding migration can be difficult to control a nerve injury and bleeding cannot be managed inappropriately, blood may accumulate within the surgical site, promoting hemorrhage. This increases the pressure in the throat and can cause confusion or difficulty swallowing and breathing.
- Airway obstruction: Heavy bleeding or ongoing bleeding in the throat can cause airway obstruction. Swelling can compress pools of blood or lungs or lung contents, making it difficult for the patient to breathe, possibly requiring immediate intervention.
- Infection: Any tissue damage, especially injury to large vessels increases the risk of infection. Blood collection at the surgical site can provide a medium for bacteria to grow, leading to postoperative infections such as cellulitis or abscess. Damage to nearby structures: the superior thyroid gland is in proximity to structures important, including recurrent laryngeal vein, carotid artery, and jugular vein can cause damage, leading to vocal cords that are weakness (repeated nasal artery damage), carotid artery damage, or more vascular injury or complications.
- Venous Thrombosis: Injury to the superior thyroid vein ought to cause venous thrombosis, in particular, if the vein isn’t always well repaired or ligated all through surgical operation. This can lead to problems with bleeding in the region, strengthening of pressure, or swelling.
- Thyroid gland dysfunction: In some cases, tissue damage around the thyroid can also affect blood flow to the gland, thyroid dysfunction or ischemia is certainly the main cause, although this is rare not compared with headaches, also use anticoagulants. A thorough understanding of the anatomy of the neck was essential.
How does the superior vein appear in imaging studies like ultrasound or CT?
Veins seem differently in numerous imaging studies like ultrasound and CT because of their particular traits and the manner exclusive imaging modalities engage with frame tissues. Here’s how veins typically appear in every:
- Ultrasound (US) Appearance: On ultrasound, veins seem like anechoic (darkish) structures with properly described, smooth, and regularly elliptical or round shapes. They are usually seen as “tubes” with an empty or black middle, indicating blood drift within. The walls of veins may be slender and pliable.
- Compression: Veins may be without problems compressed by the ultrasound probe, which is used as a diagnostic function to differentiate veins from arteries. Veins generally tend to fall apart whilst strain is applied, even as arteries stay round.
- Doppler Ultrasound: When Doppler is used, blood going with the flow inside the veins can be assessed. This will show a pulsatile glide for arteries, but for veins, it’ll display a non-pulsatile, phasic waft, usually influenced by respiratory. CT (Computed Tomography) Appearance: On CT scans, veins commonly seem like low-density systems (darker areas) as compared to arteries, that have higher density due to their muscular partitions and blood go with flow. However, veins may not constantly be visible until they are filled with contrast cloth.
- Enhanced Computed Tomography: When evaluation dye is injected, veins grow to be extra seen. The comparison fills the veins, making them seem like tubular systems with a comparison-superior center, which is lighter than the encircling tissue. The veins are regularly visible as more irregular compared to arteries and may display varying diameters depending on the area.
- Thrombosis/pathology: It is Seen as a venous filling defect (a dark area where the contrast agent does not flow) in cases of venous thrombosis, indicating the presence of vascular occlusion. Overall, ultrasound is particularly effective for visualizing superficial veins and monitoring blood flow, especially when a pathology such as deep vein thrombosis (DVT) is suspected.
What are the signs of thrombosis or obstruction in the superior thyroid vein?
Thrombosis or obstruction of the top thyroid gland also can cause an extensive variety of scientific signs, although they vary in severity. Common signs and symptoms consist of: Neck swelling: This can also result from bleeding within the pancreatic lymph nodes and can also show up as domestically seen aches or lumps in the location of the thyroid gland or neck has: or aches or tenderness in the neck, mainly the thyroid glands around the encompassing regions.
- This can include muscle stiffness and muscle stiffness.
- Voice changes: May recur due to proximity to or from the larynx or hoarseness or difficulty in speaking.
- Shortness of breath (shortness of breath): If the obstructed muscle affects the air passing through the upper respiratory tract, it can make breathing difficult, especially in severe cases,
- muscle dilatation: It seems the arteries in the neck dilate because the obstruction is responsible for the return of blood flow to the surface. Increased arterial pressure: A symptom of elevated arterial pressure is swollen veins visible on the back of the neck.
- Symptoms of thyroid dysfunction: Although rare, symptoms of thyroid dysfunction (such as hyperthyroidism or hypothyroidism) can occur if the obstruction is related to thyroid issues.
- Headache: In some cases, increased venous pressure can lead to a headache, especially if the blockage affects the brain’s venous drainage. If these signs are present, medical evaluation, including imaging (like Doppler ultrasound or CT scan), is necessary to confirm the diagnosis and guide treatment.
What measures should be implemented to prevent injury to the superior thyroid vein during surgical procedures?
Many precautions must be taken when performing primary thyroid or neck surgery to avoid damage to the superficial thyroid gland:
- Anatomy and preoperative planning: Surgeons must have a thorough understanding of the anatomy of the entire neck, including the course of positive thyroid vessels and their relationships with others present carotid artery, and pulmonary recurrence. Preoperative imaging (inclusive of ultrasound or CT scan) can help pinpoint the exact place and vascular modifications. Gentle cuts: When working within the thyroid and neck region, cautiously cut gently to avoid inadvertent tissue harm. Aggressive incisions with a glove or blunt device can help appropriately reveal the surgical web page without unfavorable soft tissue.
- Identification of Veins: During surgery, veins, which include the superior thyroid vein, need to be diagnosed early within the system. Meticulous care should be taken whilst manipulating or ligating the veins, specifically if they may be large and draining at once into the inner jugular vein.
- Electroplating and use of hemostatic agents: If electrolysis is used, ensure that it is applied only to tissues intended to be cauterized, and avoid direct contact with tissues. Any intravenous bleeding can be controlled by using dressings or catheters in a way that minimizes the risk of injury to the surrounding structure.
- Avoid immoderate compression of the thyroid: Avoid immoderate compression of the thyroid gland or surrounding tissue, that can stretch or compress the superficial thyroid gland, causing ability damage during a surgical procedure or other oral methods.
- How to avoid burnout low strain day and controlled technique team conversation: Surgeons and assistants ought to talk whilst standing, in particular, whilst pots are near big motors in operation.
Following these precautions can minimize damage to the upper thyroid gland during surgery, reducing complications such as bleeding or tissue damage.
What is the size of the thyroid gland, and what is its common name?
There are total three thyroid glands, making a total of six thyroid glands. They are nomenclature based on their anatomical rank comparable to the thyroid gland in humans. Here’s a breakdown:
Superior Thyroid Veins (Pair)
- Right Superior Thyroid Vein
- Left Superior Thyroid Vein
Details on Each Pair:
- Superior Thyroid Veins:Function: Drain the thyroid gland’s additional portion.
Superior Thyroid Veins:
- Location Relative to Thyroid Gland: The superior thyroid veins are located superiorly (toward the top) relative to the thyroid gland. They drain the upper section of each thyroid lobe of the gland by themselves.
- Course: These veins travel upward from the thyroid gland and typically follow a path along the lateral aspect of the thyroid lobes before emptying into the internal jugular veins. The superior thyroid veins in human thyroid glands are found on the sides of the gland where they are most abundant.
- Right Superior Thyroid Vein: According to human anatomy, the right superior thyroid vein drains the top portion of the right lobe of the thyroid gland.
- Left Superior Thyroid Vein: The left superior thyroid vein in humans is responsible for draining the anterior part of the thyroid gland’s left lobe.
- Path: After leaving the thyroid gland, these veins often empty into the internal jugular veins. The large veins in the neck carry blood from the head and neck, where there is a lack of oxygen in the body, to the heart in the body.
- Summary of Anatomical Relationships- Superior Thyroid Veins: the superior thyroid’s veins further, The internal jugular veins get drainage from the top component of the thyroid lobes, which is positioned above the thyroid gland.
What effect does thyroid revascularization have on the system as a whole?
The thyroid veins play an essential function inside the overall venous return device by facilitating the drainage of blood from the thyroid gland and contributing to the return of blood to the coronary heart. Here’s an in-intensity study of their contribution: Drainage of Blood from the Thyroid Gland- Function: The thyroid veins’ primary fragment is to empty deoxygenated blood from the thyroid gland in human frame structure. This blood includes metabolic waste products and thyroid hormones which have been released into the bloodstream.
Are there any specific imaging challenges associated with thyroid veins?
Yes, imaging challenges can include differentiating between veins and other structures due to their proximity and size. Small or variably positioned veins may be difficult to visualize clearly, requiring advanced imaging techniques for accurate assessment.
Are there specific techniques to visualize thyroid veins in difficult cases?
Advanced imaging techniques such as high-resolution ultrasound, contrast-enhanced CT, and MRI are used to better visualize thyroid veins, especially in complex cases where standard imaging might be insufficient.
What should patients know about thyroid vein issues before thyroid surgery?
Patients should be aware that thyroid vein anatomy may affect the complexity of the surgery and recovery. Discussing potential risks and ensuring detailed preoperative imaging can also help in planning and minimizing complications.
How is the superior thyroid vein ligated during a thyroidectomy?
During thyroidectomy, ligation is an important step to control bleeding and ensure a normal surgical outcome. The most common types of ligaments during thyroidectomy are the superior thyroid, the middle thyroid, and the inferior thyroid depending on the extent of the surgery Here is an explanation of how to make a ligature:
- Identify the tissues: Dr. A. The surgeon first identifies the facial nerve surrounding the thyroid. The inferior thyroid gland fills in the missing portion, the middle thyroid gland replaces the middle portion, and the anterior thyroid gland completes the upper portion of the thyroid. Careful dissection facilitates decreased damage to important systems along with the pulmonary regurgitation and parathyroid glands.
- Vein closure: Once the vein is uncovered, it’s far tied (closed) with sutures, sutures, or other hemostatic gadgets. The veins are ligated to prevent bleeding at some point in surgical treatment.
- Superior thyroid vein: This is usually ligated at its origin near the junction of the internal gagular vein and the common carotid artery. Middle thyroid vein: This vein runs into the internal jugular vein and can be ligated during surgery.
- Inferior thyroid artery: If the lower part of the thyroid needs to be removed or there is a large artery below the thyroid, the inferior thyroid artery is usually attached.
- Bleeding: After ligating the artery, the surgeon checks for bleeding, checks for bleeding, and stops before performing the rest of the operation. Tethering is essential to reduce postoperative complications such as bleeding or excessive bleeding, and to optimize patient recovery. The exact method of combination may vary depending on the individual case and the surgeon’s preference.
What is the significance of the superior thyroid vein in central line placement or neck vascular surgeries?
- The superior thyroid gland plays an important role in central nerve fixation and peripheral nerve surgery, especially in location and proximity to vital systems in the neck To assess the upper body’s lower extremities, it is important to minimize the risk of complications in time Central implant placement. If these vessels are inadvertently punctured or damaged during the procedure, bleeding or bleeding may occur.
- Glandular differences: The thyroid gland is anatomically different from the gland. In some individuals, the superficial thyroid gland may be enlarged or exposed, so care must be taken to avoid accidental injury during midline insertion.
- Vascular surgery of the neck: Surgical risks: During neck surgery such as thyroidectomy or carotid artery surgery, the superior thyroid gland is often encountered and surgeons should be careful with this gland to avoid hypertension or unintentional injury. Damage to the superficial thyroid gland can lead to postoperative complications such as hematoma or seroma formation.
- Ablation considerations: For surgeries that involve glands such as the thyroid, parathyroid gland, or carotid artery, ligation or retraction of the superior thyroid artery may be necessary, surgeons must ensure careful handling of this vein to avoid unnecessary bleeding and proper identification of the surgical site continue to be held as. In summary, the superior thyroid vein is significant in both central line placement and neck vascular surgeries because of its anatomical proximity to important structures like the internal jugular vein, carotid artery, and thyroid gland. Proper knowledge and care are needed to avoid complications during procedures in the neck region.
Can the superior thyroid vein be involved in systemic venous diseases, such as thrombophlebitis?
Yes, an increased thyroid gland can be used in thrombophlebitis and other vascular sicknesses, although it is uncommon. Thrombophlebitis refers to inflammation and bleeding in the head, which usually influences the decreased extremities, however can also affect the veins of the pinnacle and neck, which includes the higher thyroid gland.
The upper thyroid gland drains blood from the thyroid gland and surrounding systems, normally in the internal jugular vein If a thrombus (clot) forms within the top thyroid gland, it can local infection, aches, swelling, or possible headaches including even hazard of embolism may be associated with will increase the chance of thrombosis (DVT), or blood clots which include sure cancers, excessive bleeding, or contamination. However, tissue-precise thrombophlebitis is extremely uncommon. Involvement of a superficial thyroid gland tended to motivate localized signs in the neck vicinity.
What role does the superior thyroid vein play in thyroid-related tumors or goiters?
The superficial thyroid gland plays an important role in the nerve supply of the thyroid gland, but its involvement in tumors or thyroid-related tumors is more abnormal Function and relevance in different conditions among these: It is responsible for absorbing the intestines The intestines usually empty into the jugular vein. It helps remove deoxygenated blood from the thyroid and surrounding structures in the middle and lower thyroid glands.
- Thyroid tumor or goiter: Although the superior thyroid gland itself does not directly contribute to the development of a thyroid-related tumor or goiter, its function is important during surgery or when the thyroid is enlarged due to a goiter or tumor. Increased arterial pressure: In the event of a goiter or a large thyroid tumor, the nerve supply to the thyroid gland can be damaged or altered, causing increased arterial pressure This can cause swelling of the arteries, affecting the thyroid superficial nerves, causing problems or complications.
- Surgical considerations: Surgeons should monitor the upper thyroid gland closely to avoid hypertension during surgery to remove a thyroid tumor (such as thyroid cancer) or to treat goiter Typically the gland is tied (tied). And to prevent postoperative bleeding, as it is the main route for venous drainage.
- Tumor metastasis and its dissemination: In some cases, especially with thyroid cancer, lymph nodes linked to carcinoid tumors (found in the upper part of the thyroid) can act as routes for cancer cells to travel, although the surrounding muscles contribute to the importance of the tumor, which further aids in its proliferation.
Overall, although elevation of the thyroid gland is essential for normal thyroid regeneration, the use of surgical intervention is closely related to its role in thyroid tumors or cysts and their appearance well that the stress veins will be propagated in the wider cases.
Are there congenital abnormalities associated with the superior thyroid vein?
Yes, congenital higher thyroid nodules, however, it could happen. These abnormalities are often related to thyroid gland changes and can be related to anatomical differentiation or developmental abnormalities, Congenital abnormalities of the higher thyroid gland include:
- Absence or hypoplasia: In a few cases loss of one or superior thyroid glands. Venous outflow to the thyroid gland may be affected, inflicting Obstruction or different headaches.
- Drainage differences: The superior thyroid vein usually drains into the peripheral nerve, but in some individuals other veins such as the brachiocephalic vein or posterior. These changes can be asymptomatic but can be significant in surgical procedures such as thyroidectomy.
- Multiple superior thyroid glands: Some individuals may have more than one superior thyroid gland on one or both sides. Although this is rarely a problem, it can complicate surgery and requires careful identification of vessels during surgery.
- Abnormal communication: Rarely, there can be communication or abnormal communication between the superficial thyroid gland and other glands, such as the deep cervical artery or the common carotid artery These abnormalities are often found incidentally and are usually asymptomatic but can complicate surgery in the neck region.
These congenital abnormalities are often discovered incidentally during imaging studies or surgery. It is usually not associated with significant clinical symptoms except to prevent vascular permeability or to complicate surgical procedures.
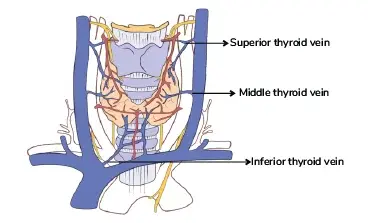
How do the superior thyroid glands compare with other thyroid glands (e.g., middle and inferior thyroid glands)?
Along with the center and inferior thyroid glands, the superior thyroid gland is a part of the frightened device that ends in the thyroid gland. This is the assessment: superior thyroid veins, or superior thyroid vein: Origin extracts blood from the larynx, throat, and surrounding regions, including the pinnacle thyroid gland. Of course – connects to the thyroid gland and its surface is usually similar, and it runs down and out of the thyroid gland. Drainage: Typically, it enters the jugular vein (IJV) at the cricoid cartilage level. Size: The thyroid is usually the smallest of the glands and first secretes blood from the thyroid gland. Middle thyroid vein: Initially drains the middle portion of the thyroid gland. The lesson is that the inner jugular vein is drained by the central thyroid gland, which goes upward.
Infiltration: vein usually infiltrates the inner lung tissue at a lower level than the superior thyroid gland. Size: The central thyroid gland tends to be of different size compared to the superficial gland. Inferior Thyroid Vein: Origin Draws blood from the base of the thyroid gland and the surrounding tissues. Action: Descends into the brachiocephalic vein (sometimes directly into the left innominate), usually inferiorly to the superior and middle thyroid glands: The inferior thyroid gland has a larger caliber than the superior central artery, which reflects the amount of blood from which the lower portion of the artery.
Comparison General Summary: The lower thyroid gland is usually characterized by largest, followed by the middle thyroid gland, with the superior thyroid gland being much smaller. Urine: The superior thyroid gland drains into the jugular vein at the top of the neck, while the inferior thyroid gland drains into the brachiocephalic vein at the base of the neck. It drains the upper thyroid lobe, the middle vein drains the middle, and the lower vein drains the lower thyroid lobe. In summary, the thyroid gland is similar in that it supplies parts of the thyroid gland, but it differs in size, the direction of flow, and infiltration.
Are there any differences in the superior thyroid vein between individuals or across populations?
The superficial thyroid gland (STV) might also range slightly in its anatomy between individuals or populations, even though its universal structure stays the same where the superior thyroid vein drains the thyroid gland and often is positioned on the junction of the internal jugular vein with the subclavian vein however may additionally fluctuate in several approaches: range of branches; Some individuals may also have multiple elevations of the thyroid glands on each aspect, while others might also have an unmarried gland that drains the thyroid gland This may vary depending on the scale of the thyroid gland or if there may be a glandular leak it can not exist.
Venous drainage pattern: Although the superior thyroid vein usually drains into the internal jugular vein, it can sometimes drain directly into the brachiocephalic vein or other systems depending on the individual In some cases, the superior thyroid vein may anastomose and middle thyroid vein or inferior thyroid vein There is a change in the rate of drainage. Length and Course: STV’s course may vary slightly.
In some individuals, the nerve takes a more direct route to the internal jugular vein, while in others it takes a longer or more curved route Physiologic changes in the surrounding environment may be affected. The length of the superior thyroid vein. Population differences: Although most studies suggest that the overall anatomy of the upper thyroid glands is fairly consistent across the population, some ethnic and regional variations have been observed e.g. You can’t listen to that thyroidectomy but these know that changes can be necessary for certain treatments or studies.
Disclaimer:
The information provided about the superior thyroid vein is for educational purposes only. Although efforts were made to ensure the accuracy of the data, physiological changes and treatment conditions may cause differences in tissue structure and function. For any medical concerns or diagnoses, it is crucial to consult a licensed healthcare provider. This information is not intended to replace professional medical guidance, diagnosis, or therapy.
Important Considerations:
- Consult with Medical Experts: For any health concerns or conditions associated with the thyroid vein, including those that necessitate diagnosis, treatment, or surgical procedures, it is essential to obtain advice from a qualified healthcare professional. This information is just for informative purpose don’t depends on it. It’s just a detail of superior thyroid vein.
- Liability: The creators and distributors of this information are not liable for any errors, omissions, or outcomes that may arise from the use or interpretation of this content. Choices about medical treatment ought to be determined after discussions with a healthcare provider.
- Nothing Substitutes for Professional Advice: Content should not be used as a substitute for the provision of medical advice, diagnosis, or treatment. Continue to seek guidance from your doctor or other qualified healthcare provider with any questions you may have about medical illness or treatment.
By using this knowledge, you acknowledge and agree that it is for educational purposes only and does not constitute medical recommendations.
FAQ
What is the ideal thyroid pulse?
The superior thyroid vein is a blood vessel that drains blood from the thyroid gland, including the superior portion.
What is the feature of the superior thyroid gland?
The superior thyroid gland is accountable for pumping oxygen-poor blood from the thyroid gland and adjacent glands. This blood is then again sent to the ordinary circulatory gadget via the peripheral arteries.
Where do the superior thyroid glands drain?
The higher thyroid gland typically connects to the internal lymph nodes, which convey blood to the heart. It can also occasionally drift immediately into the brachiocephalic vein.
What are the possible complications of the superior thyroid vein?
Injury during surgery: Damage to the upper thyroid gland during a thyroidectomy (removal of the thyroid gland) can cause significant bleeding. Venous thrombosis: Although rare, blood can form in the vein, causing an area of swelling and possible complications.
How is hyperthyroidism related to blood flow to the thyroid vein?
While the superior thyroid gland drains blood from the thyroid gland, the blood comes from the superior thyroid gland itself, which is a branch of the external carotid artery artery with good circulation with the thyroid gland which is important for muscle of function and health.
Does the superior thyroid vein have any role in endocrine function?
Higher thyroid glands do not contribute directly to the endocrine function of the thyroid, including hormone secretion (such as thyroid hormones T3 and T4) but their role in blood cleansing promotes normal thyroid gland anatomy so stay there.
Reference
For specific facts about superficial thyroid glands, you can also refer to the following books on anatomy and scientific anatomy: Gray’s Anatomy: Anatomic Basis of Clinical Behavior. This traditional description of anatomical variation hormone plays a role for humans, thick muscles in the neck muscles and tendons in the body. Clinically Oriented Anatomy by Keith L. Moore, Arthur F. Dalley, and Anne M. R. Agur This book is highly regarded for its clinical approach to anatomy and offers clear explanations and illustrations of the vascular structures, including the thyroid veins. Arthur C. Guyton and John E. McCarthy.
While Hall’s textbook of medical anatomy is primarily an anatomical treatise, Guyton’s work contains relevant information on the thyroid blood circulation and the tissues from which it Anatomy of the Human Body By Henry Gray (Bartlett & Treadgold’s) This edition presents comprehensive anatomy of the body and a description of the known nervous systems thanks to its accurate and colorful illustrations, this atlas provides detailed anatomy that can help visualize the superficial thyroid gland about other structures These books provide in-depth information that should help understand superficial anatomy of body and related under clinical for.