
Supraspinatus muscle
What is the Supraspinatus muscle?
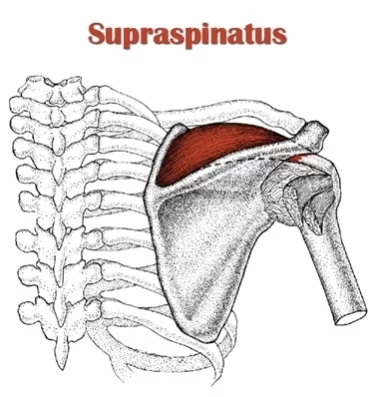
The supraspinatus muscle is one of the four rotator cuff muscles located in the shoulder. It is responsible for initiating the abduction of the arm and stabilizing the shoulder joint during arm movements. Injuries to this muscle can result in shoulder pain and limited mobility.
Along with the infraspinatus, teres minor, and subscapularis muscles, the supraspinatus is one of the rotator cuff muscles. The supraspinatus muscle extends from the supraspinous fossa of the scapula to the proximal humerus and is deep within the trapezius muscle in the posterior scapular region.
Along with the other rotator cuff muscles, the supraspinatus stabilizes the glenohumeral (shoulder) joint during the actions of the upper limb. Moreover, it aids the abduction of the arm.
Origin of Supraspinatus muscle
scapula’s supraspinatus fossa. a shallow depression in the scapula’s body above the spine.
Insertion
The superior facet of the humerus, (a greater tuberosity).
Relations
The supraspinatus muscle is located above the scapula’s spine and deep beneath the trapezius muscle. The subacromial bursa separates the supraspinatus tendon from the coracoacromial ligament, acromion, and deltoid muscle.
Innervation
The anterior rami of spinal nerves C5 and C6 form the suprascapular nerve, which innervates supraspinatus.
Blood supply
The suprascapular artery, which is part of the thyrocervical trunk of the subclavian vein, supplies the supraspinatus with blood. The suprascapular artery and nerve supply the supraspinatus through the suprascapular notch.
The dorsal scapular artery provides the supraspinatus with collateral blood supply on occasion. Venous waste is conveyed by the equivalent named veins which go with the arteries and drain into the subclavian vein.
Function of Supraspinatus muscle
The supraspinatus muscle contributes to the stabilization of the humeral head in the glenohumeral joint during movements. Additionally, it aids the deltoid muscle in the glenohumeral joint’s abduction of the arm.
Clinical significance
One of the rotator cuff’s most frequently damaged parts, the supraspinatus is a part of the rotator cuff and can be injured suddenly or slowly. Unsympathetic partial and full tears, as well as symptomatic syndromes with chronic pain, are among the leading risk factors, as are age and poor posture. Associated pathologies contain acromial impingement, frozen shoulder, and poor sleep habits, particularly as an afterthought. MRI and ultrasound are now useful diagnostic tools.
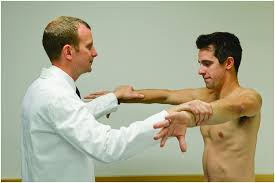
Test for Supraspinatus:
A common orthopedic examination test for supraspinatus impingement or the integrity of the supraspinatus muscle and tendon is the Full Can Test in conjunction with the Empty Can Test. Sitting or standing usually makes the test easier. The shoulder girdle is stabilized by one of the examiners on the side that will be tested. The arm to be tried is moved into 90 levels of abduction in the plane of the scapula (roughly 30 levels of forward flexion), full internal rotation with the thumb pointing down as though emptying a beverage can. The patient resists the downward pressure applied by the examiner’s other hand to the superior aspect of the distal forearm. If there is a lot of pain and/or weakness, the Empty Can Test is positive.
Supraspinatus muscle stretching
Single-side Stretch
Stand straight with your arms hanging close by.
Put your right hand behind your back and try to grab your left wrist.
Relax your neck and tilt your head to the right for more intensity as you use your left hand to hold your wrist behind your back.
Maintaining a relaxed left shoulder, use your right hand to pull your wrist up to your back while holding it behind you.
Before moving on to the other sides, hold it for 30 seconds and do it four more times.

Supraspinatus muscle strengthening exercise
Pull back press
This is a strengthening exercise for the shoulder external rotators and scapular retractors. Tie a band around a dumbbell to secure it to your feet. Pull the band back to your shoulders by grabbing both ends with your hands. By keeping your forearms parallel to the ground, you can keep your elbows stacked just below your wrists. Lift your hands over your head without permitting your hands to move advances compared with your elbows.
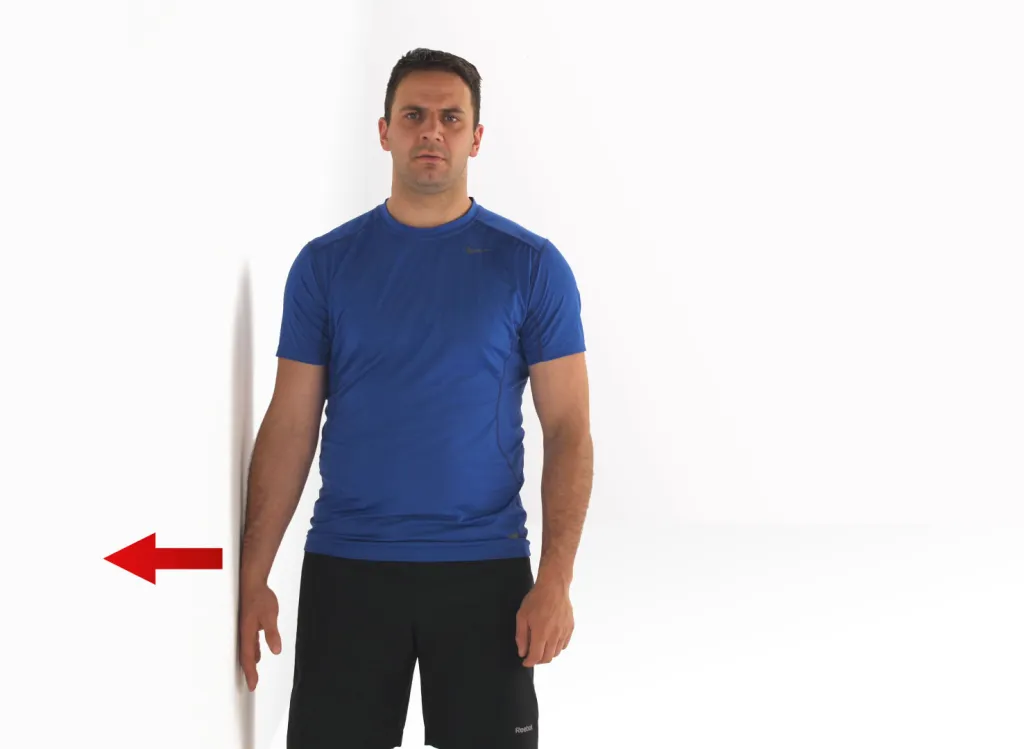
Isometric shoulder abduction
This is a work-based isometric constriction practice that utilizes a wall. With your elbows straight, stand next to a wall. To target the rotator cuff, abduct the shoulder by no more than 30 degrees. With your palms confronting your body, press outwards into the wall by gradually increasing your power over 3 seconds. Maintain your maximum tolerable contraction for 5-7 seconds before gradually decreasing your strength to rest (again over a count of three seconds).
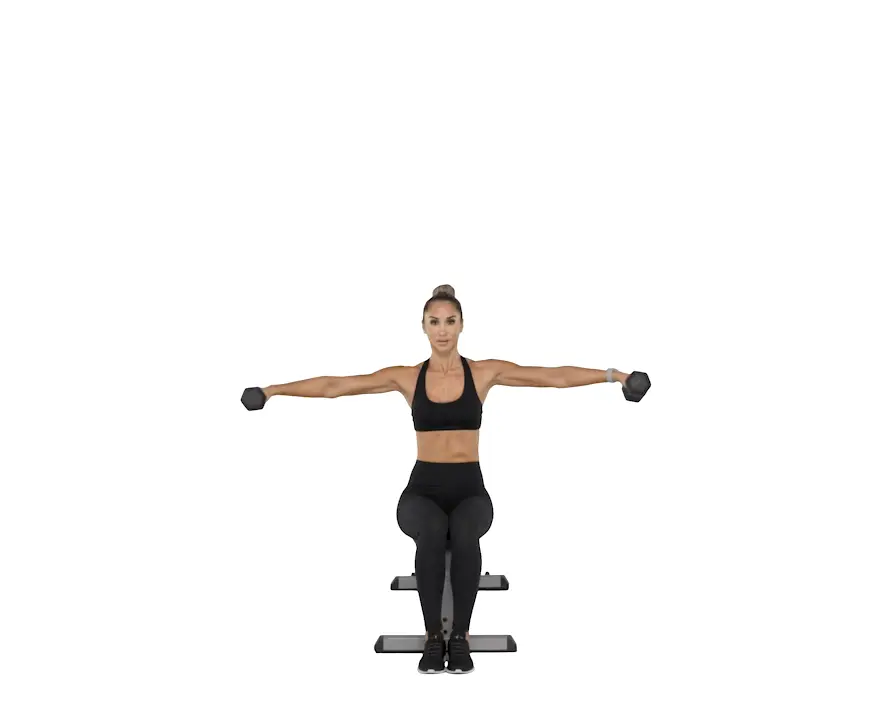
Seated lateral raise
This is a situated horizontal raise practice that will boost the muscles of the shoulder. While raising the arms, the seated position helps to isolate the movement to a pure shoulder exercise by reducing the use of full body momentum. To target the larger muscles of the shoulder, tighten the grip or loosen it to increase rotator cuff engagement.
Hanging lateral raise
This is a strengthening exercise for the upper trapezius and lateral deltoid. Lean to one side while holding a stable pole, door frame, or squat rack. Raise the arm 30 degrees in front of the body in the scapular plane. Slowly lower the arm as you raise it to about shoulder height. The side lean is used in this exercise to make more workable shoulder abduction.

Full can raise
The standard lateral raise exercise has been modified for this exercise. Begin with your arms in the scapular plane (arms around 30 degrees before your body). Lift two dumbbells to about shoulder height while holding them in a thumbs-up position (mid-pronation). During this exercise, use as little momentum as you can.

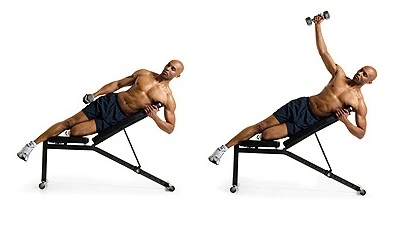
Incline side half lateral raise
The rotator cuff muscles are the focus of this strengthening exercise for the shoulder abduction. To get started, incline a bench about 45 degrees. Lie on your side on the bench, with the target shoulder facing up. Holding a dumbbell, raise it from the side of your body until it is roughly at your shoulders’ level. Bring down the load back to your side and recount as required.
Banded lateral raise
This is a strengthening exercise for shoulder abduction. Begin with your arms in the scapular plane (arms around 30 degrees before your body). Step inside a pullup, hold the band with both hands in a thumbs-up grip (mid-pronation), and then perform the exercise. Obtain your hands up to about shoulder height. During this exercise, use as little momentum as you can.

Front band pull shoulder rotations
This is a warm-up exercise for shoulder mobility. Attach one end of a light-strength band to a stable object in front of you and loop it around the upper arm close to the armpit. Have your arm raised to 90 degrees abduction and turn the arm all over to the most extreme average reach.
Horn blowers plate perturbation
This is a shoulder and rotator cuff muscle stability and proprioception exercise. First, loop the end of a band through a fractional weight plate after anchoring it to a stable object. Take hold of the other end and face the anchor point of the band with your body. To perform shoulder abduction and elbow flexion, raise your elbow to 90 degrees. To increase the band’s tension (thereby providing resistance to external rotation), step away from the band’s anchor point. Utilize your free hand to pull on the weight plate and let go to permit it to shake the band. Resist the resulting movement to stabilize the shoulder.
Powell raises
This is a shoulder abduction-boosting exercise that is utilized to focus on the deltoids. Begin by inclining a bench about 30 to 45 degrees. Lie on your side on the bench, with the target shoulder facing up. Holding a dumbbell, raise it from the side of your body until it is roughly shoulder abducted at 90 degrees. Lower the load down towards the floor before you.

Dowel shoulder abduction
A dowel is used in this shoulder abduction mobility exercise. Hold a dowel with both hands while lying on your back. Push the target hand into tolerable shoulder abduction with the healthy arm. Return to the starting position after holding the end range for up to ten seconds.
Reactive lateral catch
This is a rehabilitation exercise for the late stage of the rotator cuff that strengthens the shoulder and improves joint proprioception. Grip-based activities have been shown to increase muscle activity in the rotator cuff. By stressing the shoulder joint repeatedly while gripping and relaxing the hand in a ball drop and catch motion, this exercise takes advantage of this mechanism. The horizontal catch position is utilized to focus on the supraspinatus muscle concentrically and the other rotator sleeve muscles as co-stabilizers of the glenohumeral joint.
Shoulder abduction press
This is a changed form of the shoulder press exercise to raise shoulder strength. Attach a band to a stable object beside you at shoulder height. Holding the band next to your shoulder while pressing upwards is the first step.
Armbar
The goal of this closed kinetic chain exercise is to improve shoulder stability. Begin by holding a load with a straight arm right about your shoulder while laying on your back. By rolling your entire body away from the raised arm, you can move into a side-laying position. During this movement, zeroing in on keeping your arm as opposed to the floor as possible is significant. moves slowly into the starting position, and then does it again.

Z press
This exercise is a more advanced version of the standard shoulder press. You must sit on the floor, not a bench or chair, for this exercise. Sit with your legs straight out in front of you and wide open to better support your body. Each hand should be holding a weight, and you should move with precision. Keep the elbows straightforwardly inline and underneath the wrists consistently.

FAQ
What causes supraspinatus injury?
A partial or full-thickness supraspinatus tear can result from trauma or repeated micro-trauma. The tear usually appears as an avulsion from the greater tuberosity or as a tear in the tendon. The tear can be fractional or full-thickness.
How is supraspinatus treated?
Physical therapy, ice treatments, nonsteroidal anti-inflammatory drugs (NSAIDs), and rest are all part of this treatment. Physical therapy can also be used in conjunction with corticoid injections. If conservative treatment fails to improve after three to six months, surgical intervention may be an option.
Is tearing the supraspinatus serious?
Talk to your orthopedic surgeon if you start experiencing more pain after being diagnosed with a partial-thickness tear. Full-thickness tears typically necessitate surgery and a more aggressive treatment plan due to the complete disruption of the supraspinatus muscle fibers.
Is a supraspinatus tear capable of self-healing?
Even though the majority of tears cannot heal on their own, it is often possible to regain function without surgery. However, because many tears cannot heal without them, surgery is typically recommended if you are physically active, use your arm for sports or overhead work, or both.
What size supraspinatus tear requires surgical repair?
These are additional indications that surgery might be a good choice for you: Your symptoms have persisted for six to twelve months. You have a large tear that is over 3 cm in diameter, and the tendon tissue that is surrounding it is of good quality. Your shoulder is severely weakened and no longer functions properly.




6 Comments