Voluntary Control Grading
Voluntary control grading typically involves evaluating the individual’s ability to voluntarily initiate, sustain, and coordinate movements in specific body parts affected by spasticity or motor impairments. It helps to determine the extent of functional limitations and provides a baseline for tracking progress or evaluating treatment interventions.
- In the case of hemiplegia, cerebral palsy, etc severe spasticity will make movements impossible, these movements can be graded with voluntary motor control.
- While moderate spasticity will allow some slow movements but they will be performed with too much effort and abnormal coordination and fine movements of the limbs especially involving the distal portion will be difficult or impossible.
VOLUNTARY MOTOR CONTROL GRADING
- 1+ – Gravity eliminated plane with 1/3rd movement possible.
- 1++ – Gravity eliminated plane with 2/3rd movement possible.
- 1+++ – Gravity eliminated plane with full range of motion.
- 2+ – Against gravity 1/3rd movement possible.
- 2++ – Against gravity 2/3rd movement possible.
- 2+++ – Against gravity full range possible.
- 3+ – Against gravity with resistance 1/3rd movement possible.
- 3++ – Against gravity with resistance 2/3rd movement possible.
- 3+++ – Against gravity with resistance full movement is possible.
- 4 – Skilled movement.
SYNERGY
- Synergy patterns are abnormal, stereotyped, primitive, mass movement patterns associated with spasticity and which can be triggered either reflexively and voluntarily. Synergy can be either flexor or extensor. They involve the action of certain muscles in a combination that gives rise to an abnormal pattern not useful for functional activities.
- In hemiparesis, there are some muscles that are always involved and which finally gives rise to a peculiar abnormal mass movement pattern and attitude that is characteristic of many hemiparesis patients.
- The spasticity invariably affects the anti-gravity muscle for reasons not clearly understood. It is however presumed that these anti-gravity muscles are relatively more stretched than pro-gravity muscles in neutral position hence stimulating the stretch reflex giving rise to spasticity.
ABNORMAL SYNERGY IN UPPER AND LOWER LIMBS :
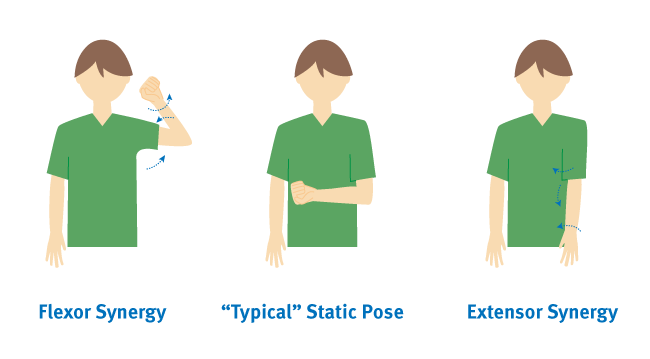
- Flexion synergy for upper limbs: Shoulder girdle retraction and elevation, shoulder abduction external rotation, supination, flexion of the elbow, wrist, and finger flexion.
- Flexion synergy for lower limbs: Hip flexion abduction and lateral rotation, knee flexion, dorsiflexion, and inversion.
- Extension synergy – For upper limbs: Shoulder girdle protraction and depression, shoulder adduction, internal rotation, elbow extension, pronation, wrist, and finger flexion.
- Extension synergy – For lower limbs :Hip extension,adduction,internal rotation,knee extension,ankle plantar flexion,inversion,and plantar flexion.
- It is highly essential to understand that synergy is different from the abnormal attitude seen in a hemiparesis patient. The abnormal hemiplegic attitude is due to the combination of the strongest component of the flexor and extensor synergy in both upper and lower limbs.
VOLUNTARY CONTROL GRADING FOR ASSESSING SYNERGY PATTERNS
- GRADE 0 : NO CONTRACTION
- GRADE 1: FLICKER OF CONTRACTION PRESENT PRESENT OR INITIATION OF MOVEMENT
- GRADE 2: HALF RANGE OF MOTION IN SYNERGY OR ABNORMAL PATTERN
- GRADE 3: FULL RANGE OF MOTION IN SYNERGY OR ABNORMAL PATTERN
- GRADE 4: INITIAL HALF RANGE IS PERFORMED IN ISOLATION AND THE LATTER HALF IN PATTERN
- GRADE 5: FULL RANGE OF MOTION IN ISOLATION BUT GOES INTO PATTERN WHEN RESISTANCE IS OFFERED
- GRADE 6: FULL RANGE OF MOTION ISOLATION AGAINST RESISTANCE.
It’s important to note that voluntary control grading is just one component of a comprehensive evaluation of motor function in individuals with conditions like hemiplegia and cerebral palsy. Other factors, such as muscle tone, reflexes, coordination, and functional abilities, are also considered to provide a more holistic understanding of an individual’s motor capabilities.
FAQs
What is voluntary control grading?
This voluntary control grade is utilized to assess the patient’s motor function. Most stroke survivors struggle to remain independent with ADLs and ambulation because of this residual impairment. The FIM scale was used to evaluate daily living activities.
How do you check voluntary motor control?
The VMC can be evaluated in stroke patients using the Fugl-Meyer Assessment (FMA). The assessment scale comprises a separate domain for balance (trunk control), upper and lower extremities (sensory and motor), and both. The motor functional tests for the upper and lower extremities are based on Brunnstrom’s stages of stroke recovery.
What is voluntary motor control?
The foundation of all exercise is selective voluntary motor control (SVMC), which is described as “the ability to isolate the muscle activity in a selected pattern in response to the demands of a voluntary motion.
What are the voluntary control muscles?
Skeletal muscles that attach to bones and can be actively engaged to govern movement are referred to as voluntary muscles. The biceps, triceps, lats, abdominals, glutes, quadriceps, and hamstrings are typical voluntary skeletal muscles.
What are the 4 levels of motor control?
Multiple structures that make up a hierarchically organised system govern every movement. From the lowest to the highest level in the hierarchy, the structures that make up the four primary tiers of the motor system are the
1) spinal cord
2) brain stem
3) primary motor cortex
4) associational cortex.

Author: Bhoomi Physiotherapist
Bhoomi Patel - Physiotherapist in Mobile Physiotheray Clinic, B - 01, Jagatnagar Society, Opp. Shaktidhara Society, India Colony Road, Tollnaka, Bapunagar, Ahmedabad.