
Erb’s Palsy & Physiotherapy Treatment:
What is Erb’s palsy?
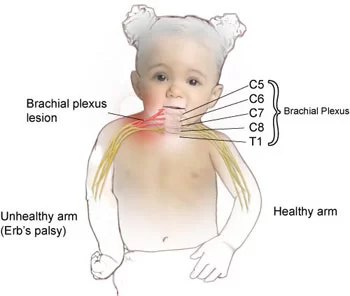
Erb’s palsy also called Erb’s Duchenne palsy is a paralysis of the arm (Upper Limb). This injury is caused mainly Due to injury to the upper group of the arm’s main nerves, Mainly the injury of the upper trunk C5–C6 nerves root. These Nerve roots form part of the brachial plexus, Forming the ventral rami of spinal nerves C5–C8 and One thoracic nerve T1.
Erb’s palsy Occurs most commonly, but not exclusively, from shoulder dystocia during a difficult birth. Depending on the nature of the damage, the paralysis can either resolve on its own over a period of months, necessary Physiotherapy Treatment, or Severe Injury May require surgical Intervention.
The paralysis can be partial or complete; the damage to each nerve can range from bruising to Complete Tear. The most commonly involved Nerve root is C5 (aka Erb’s point: the union of C5 – C6 roots) as this is mechanically the furthest point from the force of traction, therefore, the first/most affected Nerve Root. Erb–Duchenne palsy presents as a lower motor neuron Injury with sensibility Loss and vegetative phenomena.
The common nerves are involved the suprascapular nerve, musculocutaneous nerve, and axillary nerve.
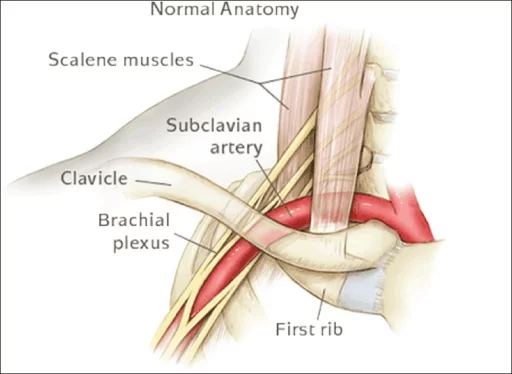
Related Anatomy
The Erb’s point, from a neurological perspective, is a location at the upper trunk of the Brachial Plexus, 2-3 cm above the collarbone. The C5 and C6 roots combine to make it, and they later converge. The axillary nerve, musculocutaneous nerve, and suprascapular nerve are the nerves that are impacted by Erb’s palsy.
The axillary nerve emerges from the posterior cord’s terminal branch, receiving fibres from C5 and C6. It passes via the quadrangular space with the posterior circumflex humeral artery as it leaves the axillary fossa in the back. It ascends to the superior lateral brachial cutaneous nerve before winding around the humeral surgical neck deep to the deltoid. It innervates the superolateral arm’s skin, the teres minor and deltoid muscles, and the shoulder joint.
The musculocutaneous nerve arises from the lateral cord’s terminal branch, which receives fibres from C5 to C7. The lateral cutaneous nerve of the forearm emerges from the axilla by puncturing the coracobrachialis, descends between the biceps brachii and brachiali while supplying both, and continues in this manner. It nourishes the skin on the lateral aspect of the forearm as well as the muscles in the anterior compartment of the arm.
The superior trunk, from which the suprascapular nerve emerges, receives fibres from C5, C6, and sometimes C4. It travels laterally through the scapular notch, inferior to the superior transverse scapular ligament, and then over the lateral cervical area, superior to the brachial plexus. The supraspinatus, infraspinatus, and shoulder joint are all innervated by it.
Epidemiology
Frequency
Brachial plexus birth palsy (BPBP) has a documented incidence of 0.8–1 per 1,000 babies in the US. About 45% of BPBP is caused by Erb’s palsy. In 20% of instances of BPBP, further damage to C7 is frequently found.
Mortality/Morbidity
3-25% of people will experience lasting disability. A good predictor of the outcome is the rate of healing over the initial few weeks. If there has been no improvement in the first two weeks of life, a full recovery is unlikely.
Race
According to a 2007 study by Weizsaeker et al, being a black person was an independent predictor for Erb’s palsy.
Sign/Symptoms
Erb’s palsy symptoms and signs include:
- Shoulder, arm, and elbow paralysis or limpness.
- Your arm or hand may feel numb or tingling. These are additionally referred to as “burners and stingers.”
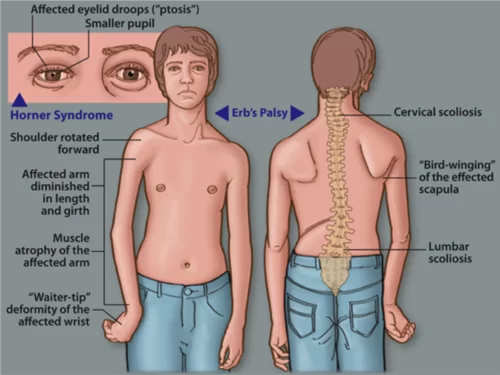
- ‘The waiter’s tip’ position of the hands.
- The elbow’s ability to bend and the forearm’s ability to supinate are both lost, making it impossible to elevate the arm from the side. The supraspinatus and infraspinatus muscles are the ones that are most frequently either partially or completely paralyzed.
The signs of Erb’s Palsy include loss of sensation in the arm and paralysis or weakness of the deltoid, biceps, and brachialis muscles. “The position of the limb, under such conditions, is by the arm hangs by the adducted and is rotated internally; the forearm is in pronation and extension position. Shoulder Abduction, elbow Flexion, and Supination is lost Mainly. The resulting Condition Look’s Like the Position also Called “waiter’s tip Hand “.
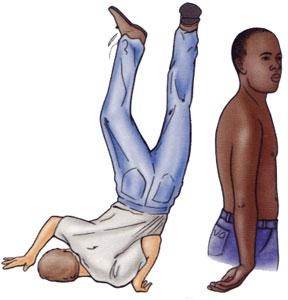
If this injury occurs at an early age may Leads to affect development (e.g. as a neonate or infant), it often leaves the patient with Delayed growth in the affected arm with everything from the shoulder through to the fingertips smaller than Compared to the Normal arm. This also leaves the patient with Delayed muscular, Nervous & circulatory development. The Delayed muscular development May lead to the arm being much weaker than a Normal one, and less articulation, with many patients unable to lift the arm above shoulder height, as well as leaving many with a Muscle contracture.
Cause:
Congenital
Dystocia ( Difficult ChildBirth-Labor)
Fracture At Clavicle to Neonates.
Any age following trauma to the head and shoulder.
Diagnosis:
Examine The Patient’s Arm Position Like Adducted From the Sholder, Extended From Elbow Joint, And Pronated Position With Weakness or Paralysis Of Deltoid, Brachialis, or Biceps Most Commonly.
Further Investigation Is By EMG/NCV Reports Or By MRI Accordingly.
Treatment:

Some babies recover on Gradually With Physiotherapy Treatment, however, Patient some may require specialist intervention or Surgical Procedure According To Injury.
Neonatal/pediatric neurosurgery is often required for avulsion Injury. Lesions may heal Naturally Over Time and function Gradually return With the Help Of Exercise Therapy.
Physiotherapy care is required Mainly to restore muscle Function. Although the range of motion is recovered in many children under one year of age, individuals who have not yet healed after this point will rarely gain full function in their arm and may develop Deformity.
The three most common treatments for Unrecoverable Erb’s Palsy are:
1. Nerve transfers (usually from the opposite arm or limb)
2. Sub Scapularis releases and Latissimus Dorsi Tendon Transfers.
Physiotherapy Treatment:

Assessment Of Patient Mainly Muscle Chart Of Whole Upper Limb And Range Of Motion And RD Test.
Accordingly, Design Treatment Plan And Monitoring Progress Report With SD Curve At Every 10 Days Helps the Recovery Process Going On.
According to the Muscle Chart Strengthening Exercise, Electrical Stimulation, Passive Movement, or Active assisted Exercise are Design.
Home Exercises are Taught To the Patient’s Relative And Deformity Correction Position And Splinting Training Are Also Required.
Mainly Aeroplane Splint Commonly Used But It May Be Vary According To Condition.

FAQs
Which nerve is affected in Erb’s palsy?
The upper trunk of the brachial plexus (C5 and C6 nerve roots) is frequently damaged in Erb’s palsy.
The axillary nerve, musculocutaneous nerve, and suprascapular nerve are the affected nerves in Erb’s palsy from the C5 and C6 nerve roots.
What are the symptoms of Erb’s palsy?
Erb’s palsy symptoms and signs include:
Shoulder, arm, and elbow paralysis or limpness.
Your arm or hand may feel numb or tingling. These are additionally referred to as “burners and stingers.”
‘The waiter’s tip’ position of the hands.
The elbow’s ability to bend and the forearm’s ability to supinate are both lost, making it impossible to elevate the arm from the side. The supraspinatus and infraspinatus muscles are the ones that are most frequently either partially or completely paralyzed.
What muscles are paralysed in Erb’s palsy?
The C5 and C6 roots of the brachial plexus are involved in Erb’s palsy, also known as Duchenne-Erb paralysis. The deltoid, biceps, brachialis, infraspinatus, supraspinatus, and serratus anterior muscles’ strength is impacted by C5 and C6 palsy.
What is the difference between brachial palsy and Erb’s palsy?
Brachial plexus palsy, which can occur during childbirth, is weakness or paralysis in sections of the arm as a result of serious brachial plexus injury. Erb’s palsy is the most common variety of brachial plexus palsy. It’s possible for childbirth to trigger brachial plexus palsy.
What is the diagnostic test for Erb’s palsy?
a test to detect Erb’s palsy
Imaging tests will be performed by medical professionals to ascertain whether your child has Erb’s palsy. These exams typically include a CT scan or an MRI scan. Most MRIs and CT scans are completed in a few hours and frequently give doctors enough data to make a diagnosis.
Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803

Arms r moving…but finger r not open.
Plz suggest me.