
Axillary Nerve
Axillary Nerve Anatomy
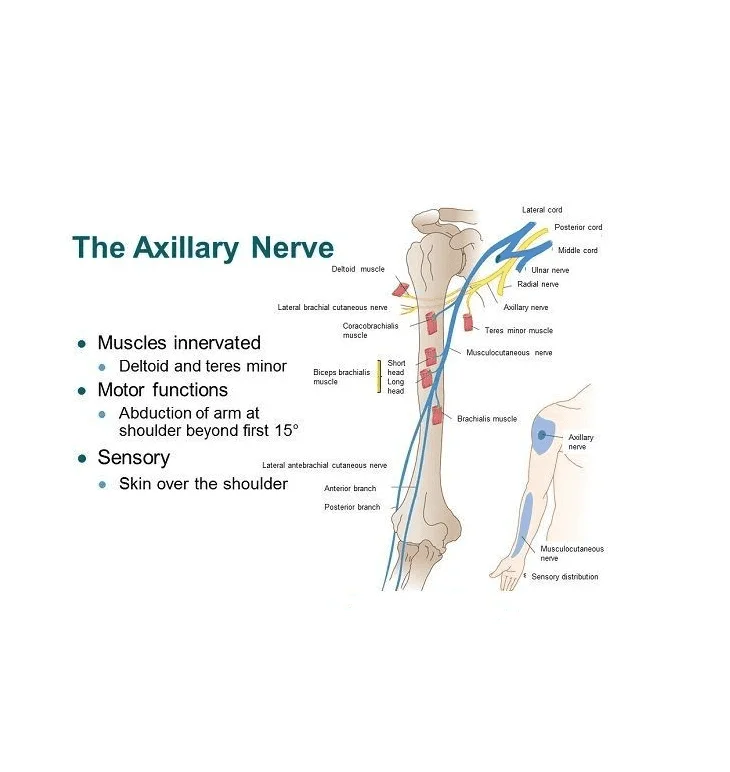
The axillary nerve originates from the ventral rami of the C5 and C6 spinal nerves and extends as the smaller branch of the brachial plexus’s posterior cord. Its anterior supply the teres minor while its posterior branches supply the deltoid muscle.
After action from the supraspinatus has already reached 15 degrees, the arm can be abducted thanks to innervation of the deltoid muscles. In addition to facilitating lateral rotation, the teres minor helps to keep the glenohumeral joint stable.
The axillary nerve’s posterior branch innervates the teres minor before giving rise to the upper lateral cutaneous nerve. The regimental badge area is the location where the inferior lateral deltoid region receives sensation from the upper lateral cutaneous nerve.
Root value:
Spinal roots: C5 and C6.
Sensory functions: Gives rise to upper lateral cutaneous nerve of arm, which innervates the skin over the lower deltoid (‘regimental badge area’).
Motor functions: Innervates the teres minor and deltoid muscles.
Description:
- The Axillary nerve (circumflex nerve), is an upper extremity nerve, which is part of the posterior cord (C5-C6), and provides motor innervation to the deltoid and teres minor muscles.
- nerve injury is characterised by trauma to the axillary nerve: from either a compressive force, a traction injury following anterior dislocation of the shoulder,or a forced abduction movement of the shoulder joint. nerve injury can cause signs and symptoms of a localized neuropathy.
Signs and symptoms may include:
- Pain to the area of the deltoid and anterior shoulder.
- Loss of movement and/or lack of sensation in the shoulder area
- Reported or observed weakness to the deltoid and teres minor muscles (Abduction and external rotation).
- A true axillary nerve injury (mononeuropathy -involving a single nerve), should not present with any changes to the local reflexes.
Anatomical Course:
- The axillary nerve is formed within the axilla area of the upper limb. It is a direct continuation of the posterior cord from the brachial plexus – and therefore contains fibres from the C5 and C6 nerve roots.
- In the axilla, the axillary nerve is located posterior to the axillary artery and anterior to the subscapularis muscle. It exits the axilla at the inferior border of subscapularis via the quadrangular space, often accompanied by the posterior circumflex humeral artery and vein.
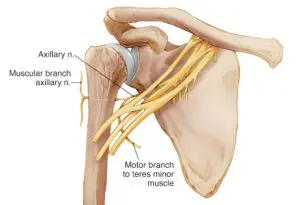
- The axillary nerve then passes medially to the surgical neck of the humerus, where it divides into three terminal branches:
- Posterior terminal branch – provides motor innervation to the posterior aspect of the deltoid muscle and teres minor. It also innervates the skin over the inferior part of the deltoid as the upper lateral cutaneous nerve of the arm.
- Anterior terminal branch – winds around the surgical neck of the humerus and provides motor innervation to the anterior aspect of the deltoid muscle. It terminates with cutaneous branches to the anterior and anterolateral shoulder.
- Articular branch – supplies the glenohumeral joint.
The Quadrangular Space:
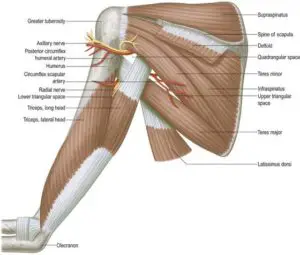
- The quadrangular space is a gap in the muscles of the posterior scapular region. It is a pathway for neurovascular structures to move from the axilla anteriorly to the posterior shoulder and arm.
- Superior – inferior aspect of teres minor
- Inferior – superior aspect of teres major
- Lateral – surgical neck of the humerus.
- Medial – long head of triceps brachii
- Anterior – subscapularis
- The axillary nerve and posterior circumflex humeral artery and vein pass through the quadrangular space.
- These structures can be compressed as a result of trauma, muscle hypertrophy, or space-occupying lesion; resulting in weakness of the deltoid and teres minor.
- This is particularly common in athletes who perform overhead activities.
Motor Functions:
- The axillary nerve innervates teres minor and deltoid muscles.
- Teres minor – part of the rotator cuff muscles which act to stabilise the glenohumeral joint. It acts to externally rotate the shoulder joint and is innervated by the posterior terminal branch of the axillary nerve.
- Deltoid – situated at the superior aspect of the shoulder. It performs abduction of the upper limb at the glenohumeral joint and is innervated by the anterior terminal branch of the axillary nerve.
Sensory Functions:
- The sensory component of the axillary nerve is delivered via its posterior terminal branch.
- After the posterior terminal branch of the axillary nerve has innervated the teres minor, it continues as the upper lateral cutaneous nerve of the arm. It innervates the skin over the inferior portion of the deltoid (the ‘regimental badge area’).
- In a patient with axillary nerve damage, sensation at the regimental badge area may be impaired or absent. The patient may also report paraesthesia (pins and needles) in the distribution of the axillary nerve.
Blood Supply
The axillary nerve emerges from the neck, passes anterior to the subscapularis muscle and posterior to the axillary artery. It approaches the lower border of the subscapularis and leaves the axilla through the quadrangular space, where it meets the posterior humeral circumflex artery and vein. The quadrangular space is bounded superiorly by the teres minor muscle’s lower border, laterally by the humerus’ surgical neck, inferiorly by the teres major muscle’s upper boundary, and medially by the triceps brachial muscle’s long head.
The posterior humeral circumflex artery and the anterior branch of the axillary nerve loop around the surgical neck of the humerus after leaving the quadrangular space posteriorly, innervating the deltoid muscle in the process. The posterior branch extends from the quadrangular space to innervate the teres minor, the skin of the lateral upper arm, and the posterior part of the deltoid.
Clinical Conditions:
Quadrangular space syndrome:
- Compression of the axillary nerve within the quadrangular space
- Overhead athletes
- Muscle hypertrophy or paralabral cysts
- Present with vague posterior or posterolateral shoulder pain
- Weakness +/- atrophy of teres minor and deltoid muscles
- Most are treated successfully without surgery but can undergo nerve decompression in recalcitrant cases
Axillary Nerve Injury:
- The axillary nerve is most commonly damaged by direct trauma to the shoulder or proximal humerus.
- Common mechanisms of injury include fracture of the humeral surgical neck, shoulder dislocation, or iatrogenic injury during shoulder surgery.
- Motor functions – the deltoid and teres minor muscles will be affected, rendering the patient unable to abduct the affected limb.
- Sensory functions – the upper lateral cutaneous nerve of the arm will be affected, resulting in loss of sensation over the inferior deltoid (‘regimental badge area’).
- Characteristic clinical signs – in long-standing cases, the paralyzed deltoid muscle atrophies, giving the shoulder a flattened appearance, and the greater tuberosity can be palpated in that area.
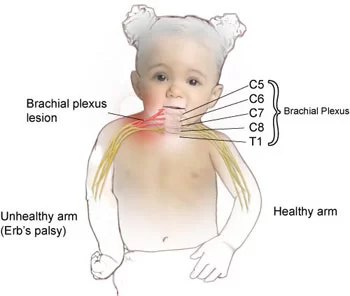
Erb’s Palsy:
- Erb’s palsy is a condition resulting from damage to the C5-C6 roots of the brachial plexus. The axillary nerve is affected, and the individual is usually unable to abduct or externally rotate the shoulder joint.
- It commonly occurs where there is an excessive increase in the angle between the neck and shoulder, which stretches (or even tears) the nerve roots.


7 Comments