

Extensor Carpi Ulnaris Muscle
What is Extensor carpi ulnaris muscle?
The extensor carpi ulnaris muscle is a muscle located in the forearm that extends from the lateral epicondyle of the humerus (a bony prominence on the outside of the elbow) and the posterior border of the ulna (one of the two bones in the forearm) to the base of the fifth metacarpal bone (a bone in the hand). It reaches up to the elbow from the base of the little finger.
Along with the anconeus, brachioradialis, extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum, and extensor digiti minimi muscles, this muscle is part of the shallow lower arm extensor bunch.
It is one of the wrist extensor muscles, which means that it is responsible for extending (bending backward) the wrist joint. The extensor carpi ulnaris muscle also helps to adduct (move toward the midline of the body) the wrist, and it plays a role in stabilizing the wrist during certain movements.
Injuries to the extensor carpi ulnaris muscle can occur due to overuse or trauma, leading to symptoms such as pain, weakness, and limited range of motion in the wrist. Treatment may involve rest, ice, compression, and elevation (RICE), physical therapy, and in severe cases, surgery.
The wrist is extended by all of the muscles in this compartment, including the extensor carpi ulnaris. Due to its particular course, this muscle also acts to adduct the hand.
Origin of Extensor carpi ulnaris muscle
The lateral epicondyle of the distal humerus and the posterior aspect of the ulna is where the extensor carpi ulnaris muscle originates.
Insertion
After passing through the sixth compartment of the extensor retinaculum, it inserts into the dorsal base of the fifth metacarpal.
Relations
The extensor carpi ulnaris muscle are the most medial muscle on the posterior forearm. The most typical portion of the normal extensor ligament is formed by the beginning filaments of the extensor carpi ulnaris, which are parallel only to the anconeus muscle and elbows at their unrivaled connection. The muscle maintains this medial position as it descends the forearm. It is restricted by the flexor carpi ulnaris, which is its forearm counterpart.
The posterior interosseous nerve (C7, C8), which is a branch of the deep division of the radial nerve, innervates the extensor carpi ulnaris. The outspread nerve comes from the back line of the brachial plexus.
Blood supply
The radial recurrent and posterior interosseous arteries, which originate from the radial and ulnar arteries, supply blood to the extensor carpi ulnaris muscle.
Function of Extensor carpi ulnaris muscle
The angled course of the extensor carpi ulnaris arranges its draw posterolaterally, making the hand expand and adduct at the same time (ulnar deviation) when contracted.
The extensor carpi ulnaris muscle, along with the extensor carpi radialis brevis and extensor carpi radialis longus, contributes to a balanced extension of the wrist that does not deviate the hand in the transverse plane. For hand-based activities like firmly clenching a fist or developing a power grip, this action is crucial. A wrist extension prevents the forearm flexors from acting on it during this process. Instead, these flexors continue to be able to only work on the digits, flexing them to form a strong grip like a tennis backhand.
Similarly, the balanced adduction (ulnar deviation) of the hand at the wrist is the result of the synergistic action of the flexor carpi ulnaris and extensor carpi ulnaris. Adduction without additional flexion or extension is that. The actions of hammering, throwing, golfing, and swinging a baseball bat all require this action. Extensor carpi ulnaris likewise adds to the solidness of the distal radioulnar joint.
Clinical Relevance
The extensor carpi ulnaris is a crucial muscle in wrist and forearm activity that helps the wrist extend and adduct as well as maintain its medial stability. It is most generally harmed by competitors subject to strong wrist developments. Tenosynovitis can develop from repetitive wrist flexion and extension due to irritation of the tendon and its sheath. Abuse can likewise prompt tendinopathy of the muscle ligament wherein there can be thickening and excruciating solidness of the ligament with insignificant primary harm. A partial tear in the tendon may result from structural damage brought on by prolonged, excessive stress on the tendon.
Assessment of Extensor carpi ulnaris muscle
A precise clinical history and evaluation are fundamental for the determination of extensor carpi ulnaris (ECU) ligament issues. Acute and chronic causes are distinguished by when symptoms first appear. In this condition, mechanical symptoms at the time of onset are also common descriptors. Patients will utilize words like snap, pop, or tear in an intense sheath disturbance.
Tendon subluxation episodes can be extremely painful in some cases. In some cases, the subluxation may not cause any symptoms at all and the patient may be able to easily replicate it. Palpation along the length of the extensor carpi ulnaris (ECU) ligament (beginning distally at its inclusion into the foundation of the fifth metacarpal to guarantee palpation of the right design) will uncover delicacy precisely restricted to that construction.
Torment on opposed dynamic augmentation with ulnar deviation is pathognomic of an extensor carpi ulnaris (ECU) condition. Pain is frequently linked to weakness. The extensor carpi ulnaris (ECU) tendon may have completely ruptured, resulting in painless weakness.
Ultrasound (US) or magnetic resonance imaging (MRI) is the imaging modality of choice to supplement the clinical diagnosis of extensor carpi ulnaris (ECU) tendinopathy and instability in ambiguous or challenging cases. Rarely are conventional X-rays required.
Treatment
Non-operative treatments for acute tendinosis of the extensor carpi ulnaris (ECU) typically include rest, activity modification, splinting (in a position of 30 wrist extension and ulnar deviation), and, on occasion, immobilization in a short-arm plaster cast for three weeks in the same position.
Strategies for rehabilitation are determined by the degree of tendinopathy. Load management and isometric exercises are used to treat the early reactive phase until the pain goes away (typically over 510 days). After that, you can gradually increase the load. During this phase, ibuprofen is thought to be helpful.
A combination of load management, eccentric work, isometrics, and strength exercises are likely to help in chronic tendinopathy when there is no sudden increase in pain.
Steroid injections into the fibro-osseous sheath should be considered if non-operative treatments do not alleviate symptoms.
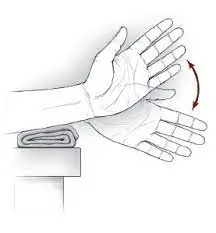
Extensor carpi ulnaris muscle stretching exercise
With your palm facing downward, extend your right arm in front of you.
Point your hand toward the ground as you bend your right arm’s wrist.
Bend your wrist even further in a downward direction with your left hand.
The stretch should be felt through your forearm’s top.
Repeat the stretch as required after maintaining it for 10 to 15 seconds.

Extensor carpi ulnaris muscle strengthening exercise
Empty Handshakes Exercise:-
You will need a table or other flat surface for this exercise.
To begin, place your forearm on the table. You can be situated or standing.
Your wrist and hand ought to be free of the table.
As if you were going to shake someone’s hand, move your hand to the side. This is where you should start.
To finish the activity, move your hand all over in a slashing movement.
Hold your movement at its highest and lowest points.
For three sets of 10 reps, complete the exercise.
Wrist Extension Exercise:-
You will need a tabletop or desk with a flat surface for this exercise. Additionally, a lightweight dumbbell between one and two pounds is required.
Standing or sitting with your feet shoulder-width apart, lay the dumbbell on the tabletop with your working hand and wrist hanging off the table in an overhand grip. Your palm ought to confront.
Pull the dumbbell up by bending your wrist upward and extending it as high as you can when you’re ready.

FAQ
How long does it take for ECU tendonitis to recover?
Healing brings two to three months for people with subluxation of the extensor carpi ulnaris (ECU) tendon and disorganization of the tendon sub sheath along the medial side of the head of the ulna. The extensor carpi ulnaris (ECU) tendon remains stable and recovers more fastly, taking four to six weeks, if the tendon sub-sheath does not divide.
Can tendonitis be permanently treated?
Rest, physical therapy, and pain medication are the most common treatments for tendonitis. Tendon tears can result from persistent inflammation. Surgery may be required for a torn tendon.
Should I massage a sore tendon?
It has the potential to alleviate pain and expedite recovery for people with tendonitis. Using a massage therapy program to relax and strengthen the inflamed tendon can improve the sufferer’s chances of a full and quick recovery from tendonitis, which can take weeks to heal.
Which medical professional treats tendonitis?
Without a medical evaluation, it is difficult to determine the severity of a tendon injury. See an orthopedic specialist for the best and most effective treatment for your joint pain.
Is ice or heat more effective for tendonitis?
For chronic tendon pain, also known as tendinopathy or tendinosis, heat may be more beneficial. Heat can increase blood flow, which may aid in tendon healing. Additionally, heat can relax muscles, which can ease the pain.



2 Comments