Ankle Inversion Sprain
What is an Ankle Inversion Sprain?
If you have an Ankle Inversion Sprain, you have damaged one or more of the 3 ligaments on the lateral side of your ankle:
- Anterior talofibular ligament (ATFL)
- Posterior talofibular ligament (PTFL)
- Calcaneofibular ligament (CFL).
A ligament’s function is to connect bones and stabilize joints. Inversion ankle sprains can potentially cause harm to the surrounding musculature and, in severe cases, a fracture.
Grades of ankle sprain
There are various grades of inversion ankle sprains.
- A grade 1– It affects only one of the three ligaments on the lateral side of your ankle with mild overstretched. A grade 1 sprain occurs when the ligament is overstretched, there is little or no ligament tearing, and the ankle stays stable.
- A grade 2– sprain occurs when one of the three ligaments is completely ripped, or when two of the three ligaments are partially torn. the ankle joint becomes unstable.
- A grade 3 -sprain causes your ankle to be the most unstable since two of the three ligaments (typically the ATFL and CFL) are fully torn.
How does this happen?
If your foot rolls inwards, it puts stress on your ankle’s lateral ligaments. The inward rolling of your foot stretches the ligaments on the outside of your ankle, which may cause them to rip. Inversion sprains are most commonly caused by landing a leap, particularly on an uneven surface such as another foot or mat, as occurs in sports such as basketball, volleyball, and gymnastics. Yet, playing sports is not the only activity that can cause a lateral ankle sprain; simple activities like missing a step or walking in an unusual way can also cause damage to the ankle.
Lateral ligaments
Inversion ankle sprains are most typically characterized by damage to the lateral ligaments. These ligaments are located on the outside of the ankle and include the anterior talofibular (ATFL), calcaneofibular (CFL), and posterior talofibular ligaments. The most common injury is to the ATFL. When both the ATFL and CFL are damaged simultaneously, ankle instability becomes more obvious. The PTFL is the strongest of the three ligaments and is seldom injured during an inversion sprain.
Ankle Sprain: Overstretched Ligaments.
Ligaments are durable rubber bands that help to stabilize any joint by limiting movement. A sprain is caused by stretching one or more ligaments beyond their usual range.
Ankle sprains range in severity from Grade I to Grade III and are valuable for more than only determining the degree of the injury; they also guide therapy and prognoses.
Introduction
Lateral ligament injuries are among the most prevalent sports-related ailments encountered by physiotherapists. Lateral ankle sprains are expected to affect men and women at roughly equal rates; however, female interscholastic and intercollegiate basketball players are thought to have a 25% higher chance of developing grade I ankle sprains than their male counterparts. In the US, around 23,000 ankle sprains occur every day, resulting in one sprain for every 10,000 people.
Lateral ankle sprains are also called supination sprains or inversion sprains. It is usually caused by a forced plantar flexion/inversion action that tears the complex of ligaments on the lateral side of the ankle to variable degrees. Although an ankle sprain is a relatively minor injury, insufficient rehabilitation can result in residual symptoms in 55% to 72% of patients within 6 weeks to 18 months. The incidence of complications and the range of long-term symptoms following an ankle sprain have led to the proposed diagnosis of sprained ankle syndrome.
Repetitive ankle sprains have been linked to functional and mechanical instability, as well as an increased risk of re-injury. Small fractures surrounding the ankle and foot (e.g., Pott’s fracture) and straining or rupture of the muscles around the ankle (e.g., calf, peroneii, tibialis anterior) should also be considered when diagnosing ankle discomfort.
Functional Anatomy:
Bones:
The ankle joint is made up of:
- Distal tibia
- fibula
- talus.
Joints:
The Ankle Complex consists of three articulations. The talocrucal (ankle joint) or Mortise joint is a hinge joint that connects the inferior surface of the tibia to the superior surface of the talus. It enables plantarflexion and dorsiflexion in the sagittal plane. The talocrural joint is supported by a joint capsule and multiple ligaments, including the ATFL, PTFL, CFL, and deltoid ligament. The ATFL, PTFL, and CFL all give lateral ankle stability.
Plantarflexion is the most unstable posture for the ankle joint, which explains why the majority of ankle injuries occur in this position.
The inferior tibiofibular joint connects the distal sections of the tibia and fibula and allows for a minor amount of rotation (in the transverse plane). Injury to these joints is known as (high ankle sprains). A thick interosseous membrane, as well as the anterior and posterior inferior tibiofibular ligaments, help to maintain the joint.
The articulation that permits eversion and inversion (frontal plane) is the subtalar joint, which is located between the talus and calcaneus. It also serves a vital purpose as a shock absorber.
The ligamentous support of the subtalar joint is substantial and is classified into three groups:
- deep ligaments
- peripheral ligaments
- retinaculr.
Ligaments of the ankle:
The lateral ligaments of the ankle are made up of the anterior talofibular ligament (ATFL), the calcaneo-fibular ligament (CFL), and the posterior talofibular ligament.
The medial (deltoid) ligament is substantially stronger than the lateral ligament and thus injured less commonly.
Muscles:
The following muscles help move the ankle joint:
- The calf group consists of:
- gastrocnemius
- soleus muscles,
- Peroneus longus and brevis,
- Tibialis anterior.
Innervation:
The lumbar and sacral plexuses supply the ankle complex’s motor and sensory functions. The tibial, deep, and superficial peroneal nerves supply the muscles with motor function. These three mixed nerves, as well as the sural and saphenous nerves, provide a sensory supply.
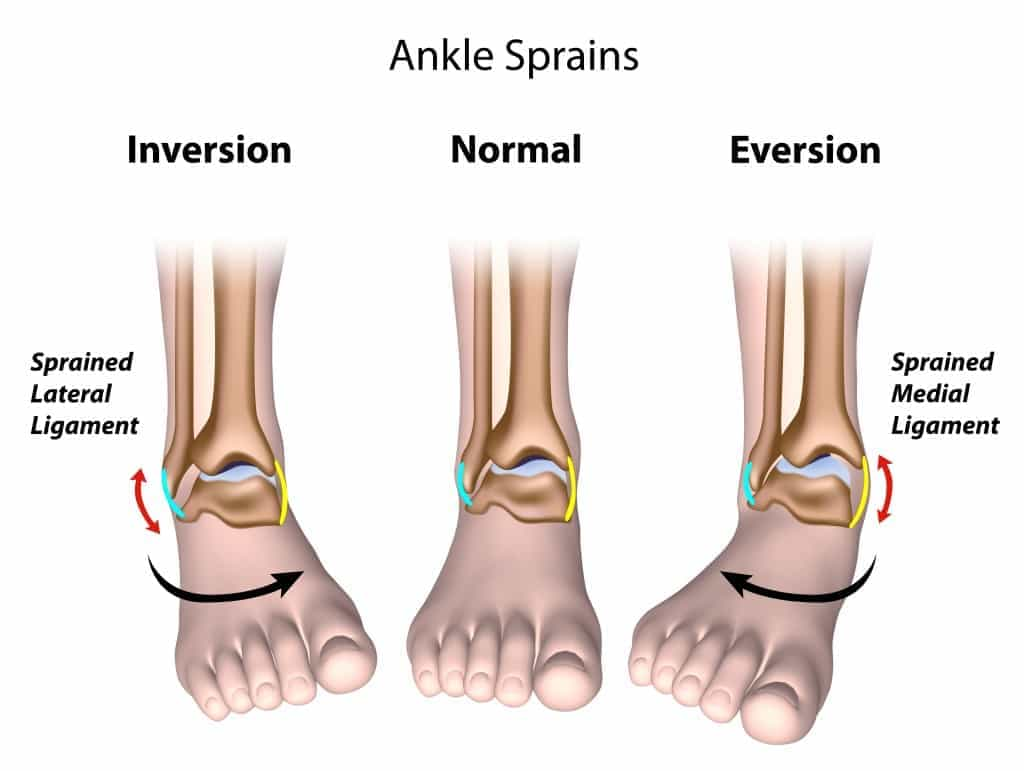
What are the Different Types of Ankle Sprains?
The ankle is one of the most stable joints in our bodies, which makes sense given that it supports our entire body weight, maintains balance, and propels or slows us down while walking or running. Although it is a very stable joint, injuries sometimes occur, the most common being ankle sprains.
Twisting and rolling one’s foot inwards and toward the body, or outwards and away from the body (inversion vs. eversion), can result in an ankle sprain. When an ankle is sprained, the ligaments stretch, resulting in decreased general balance and stability. Every stride we take prevents the ankle from rolling or twisting because of the ligaments.
Difference Between Inversion and Eversion Ankle Injuries
Inversion Ankle Injury
This type of ankle injury occurs when your foot rotates inward toward the body. This form of ankle injury occurs more frequently than eversion ankle sprains. These injuries affect the ankle’s lateral, or outside, structures, which include the anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), and posterior talofibular ligament (PTFL).
Eversion Ankle Injury
This form of injury happens when a person’s foot rolls outwards or away from their body. While not as prevalent as an inversion ankle sprain, these sprains are more serious. This is due to the fact that the deltoid ligaments inside the ankle are thicker and stronger than those outside. In other words, if this ruptures or strains, the ankle’s total instability may rise.
Risk Factors:
A lateral ankle injury was found to be significantly associated with body mass index, quick concentric plantar flexion strength, slow eccentric inversion strength, passive inversion joint position sense, and peroneus brevis reaction time.
Inversion Sprain Ankle Symptoms
When you initially roll your ankle, you will experience severe pain and be unable to bear weight on your foot (depending on the extent of the damage). Your ankle will enlarge and can get bruised. Sometimes the bruising is severe, with large areas of the foot turning purple. You may require crutches for up to two weeks to help you walk.
There may be so many bruises and swelling that you may make an indentation with your finger by pressing on the area.
Your nerves become more sensitive following a sprain. The joint aches and may throb. It’s usually worse when you press on it, move your foot in specific ways, walk, or stand.
Causes of Ankle Inversion Sprain
75% of all ankle sprains are recurrent, which implies that spraining your ankle once increases your chances of spraining it again. That is because the injury and stretch to the ligaments will mean the ankle is not supported as well in the future, making rolling the ankle more likely.
Children are frequently impacted because their balance is typically underdeveloped, and the ligaments are insufficient to maintain the ankle if it rolls badly. In addition, youngsters are prone to tumbles and falls when participating in sports. Girls are more prone to injury than males because they have more flexible ligaments, which provide less support at the ankle.
Certain sports are also more susceptible to complications. Sports that require a lot of twisting, such as netball, basketball, or field sports, might cause wear difficulties. Basketball players wear high-sided trainers to provide support for their ankle joints.
Sports on uneven ground can also be difficult, particularly on badly maintained fields. During sports, it is simple to sprain an ankle by stepping into a pothole.
Instability and degree of sprain
Ligament sprains can have the following grades:
- Grade 1- indicates mild pain and limited ligament fiber tears, whereas
- Grade 2- indicates considerable pain and extensive ligament fiber tearing.
- Grade 3: severe, sometimes painless, fiber rupture.
Mechanism of Injury
The common mechanism of a lateral ankle sprain is an inversion-type injury caused by excessive hindfoot ankle supination in an externally rotated leg. A foot in plantar flexion and internal rotation or internal rotation and mild dorsiflexion is frequently involved in inversion injuries. The entire anterolateral ankle is strained or distracted as a result, especially the calcaneofibular and anterior talofibular ligaments. These ligaments become injured, rip, or burst if their tensile strengths are exceeded.
This may result in talar tilt (calcaneofibular ligament injury) or anterolateral rotary instability (anterior talofibular ligament injury), among other complications depending on the nature of the underlying lesion.
Differential Diagnosis
It is necessary to perform a differential diagnosis in order to rule out the following less common injuries:
- Ankle fracture (distal tibia/fibular, medial/lateral malleolus)
- The medial ligament is injured.
- Ankle dislocation
- Syndesmotic injury
- Osteochondral injury
- Midtarsal sprain
Diagnosis of ankle joint
Assessment of the ankle joint
The physical examination aims to determine the:
- The degree of instability may be determined by evaluating the sprain’s grade.
- Loss of Range of motion (ROM);
- Loss of muscle strength;
- Level of reduced Proprioception.
Observation
The physical examination begins with a general assessment of the foot and ankle. Any symptoms of injury, inflammation, skin color changes, or muscular atrophy/hypertrophy are recorded. Following that, the foot and ankle are observed in two positions: non-weight bearing (n-WB) and weight bearing (WB). Make a note of the gait pattern, degree of limp (if any), facial expression on weight bearing, and any other indicators that may provide more information regarding the injury.
History
To accurately diagnose the type of damage, a history must be taken. A plantarflexion/inversion injury indicates lateral ligament damage, while a dorsiflexion/eversion injury indicates medial ligament damage. A history of injury on the same side will provide information on whether the ankle was unstable, Range of Motion (ROM).
The ankle’s range of motion should be examined both actively and passively. The movements that will be analyzed are:
Exercises include plantarflexion and dorsiflexion, as well as inversion and eversion.
Radiographic aspects
To rule out a fracture or fracture-dislocation, radiographs of the ankle are typically taken for the initial assessment of an ankle injury.
Standard radiograph
To rule out fractures, initial examinations of the ankle can be done using Mortise views, AP, and Lateral views. They could exhibit ankle swelling, a joint effusion, or an avulsion fracture.
Subtalar tilt was previously measured using stress radiographs, however, the subtalar glide test can provide clinically relevant information as well.
CT Scan
A higher-grade osteochondral injury or avulsion fracture can be better shown or detected with CT imaging.
Ultrasound
In the event of a sprain, ultrasound findings include thickening and hypoechogenicity of the damaged ligament. Anechoic defects, a loss of continuity, or the ligament’s disappearance will be visible in a tear.
MRI
MRI is frequently ordered to rule out more serious injuries or to treat persistent pain that does not improve with conventional measures. An MRI can show damage to the calcaneofibular ligament, anterior talofibular ligament, flexor, or peroneal tendons.
Moreover, MRI can rule out osteochondral, syndesmotic, and/or midtarsal joint injuries, all of which might result in treatment failure if left undiagnosed.
When evaluating the anterior talofibular ligament, axial slices or oblique axial slices with a slight anteroinferior tilt can be used to determine the ligament’s suspected course. The best ways to assess the calcaneofibular ligament are using coronal pictures and oblique axial/coronal images with a posteroinferior tilt once again in the ligament’s path.
A ligament injury may show signs of thinning, thickening, discontinuity, irregularity, or absence of the ligament. Bony avulsions are occasionally visible.
Additional soft tissue injury (strain of the muscles, peroneal tendons)
The Ottawa Ankle Rules are a helpful resource for figuring out whether you have a fracture. According to Bachmann et al.’s systematic review, there is evidence to support the Ottawa ankle criteria as a reliable tool for ruling out ankle and midfoot fractures. With the instrument’s near 100% sensitivity and moderate specificity, using it should result in a 30–40% decrease in the number of pointless radiographs.
An X-ray is recommended if a patient is not able to bear their own weight right after the accident due to the possibility of a clinically significant ankle fracture. If there are ever any legal processes, it could be important to have ignored the Ottawa standards when evaluating for ankle fractures. Although lateral ligament injuries are significantly more common, it’s important to remember that such injuries may be connected to other problems.
The so-called “problem ankle” could develop from ignoring a related injury, which could make it more difficult to recover to pre-injury functional activity levels.
Treatment of Ankle Inversion Sprain
Reduce pain and swelling
The RICE regimen (Rest, Ice, Compression, and Elevation) should be followed in order to minimize pain and edema during the initial 48–72 hours of an acute lateral ligament injury.
Elbow crutches can be given to the patient and they can be non-weight bearing (NWB) for 24 hours if weight bearing (WB) is too painful.
It is essential to initiate partial weight bearing (PWB) as soon as possible and follow a normal heel-toe gait pattern in order to reduce pain and edema.
As long as it doesn’t cause pain, light stretches and moderate soft tissue massage can help reduce swelling.
Physiotherapy Treatment
Your physiotherapist will give you exercises to help you regain the complete range of motion and strength your ankle needs to function properly as it heals. These workouts will focus on coordination, balance, strengthening, and stretching. Following an ankle sprain, the ankle frequently becomes rigid. A therapist can determine whether your ankle joint is functioning normally and, if necessary, may mobilize or manipulate it to help your ankle regain its proper function.
ROM restoration
The patient should start pain-free active range-of-motion (ROM) exercises as soon as the pain permits.
Regain strength
In particular, eversion is crucial.
Reestablish proprioception
During the rehabilitation program, proprioception training should start as soon as the patient’s pain permits.
Resuming regular activities
The following tasks should be evaluated for patients’ abilities: painless
- Twisting
- Jumping
- Hopping on one leg
- Running
- A figure of 8 running
The patient should have a full range of pain-free ankle mobility, normal strength, and normal proprioception before resuming full functional activity. If the athlete decides to resume athletics, they should be advised to tape their ankle or wear an ankle brace for an additional six months to offer external support.
When your healing is almost complete, a therapist can help you with high-intensity activity-specific exercises to make sure your ankle is prepared for whatever activity or activities you decide to undertake safely. They can also give you advice on how to prevent further sprains in your ankle.
Surgical Treatment
Acute ankle sprains can be treated surgically with arthroscopy and/or ligament restoration, depending on the circumstances, such as chronic conditions, more severe cases in sportsmen, or substantial ligamentous injuries. It is advised that the suggestion be carried out individually, with an emphasis on avoiding repetitive sprains.
Chronic ankle instability is a major aftereffect of lateral ankle sprains, especially if they occur repeatedly.
Prognosis
Thirty percent of patients suffer pain during activities 2.5 to 5 years after the acute incident, and over half of patients still experience persistent symptoms between 6 weeks and 18 months. After suffering an ankle sprain, up to 5% of athletes must alter their training regimen and up to 4% must cease all sports.
Up to 6% of non-athletes are unable to continue in their former line of work, and another 15% require extra assistance to do so. Short-term prognostic factors include functional activity score, weight-bearing, injury grade, and medium-term discomfort. Additionally, research has indicated that MRI is a reliable predictor on its own.
Complications
- Chronic ankle instability
- Chronic Ankle Pain
When there is a combined anterior talofibular and calcaneofibular ligament injury, the deltoid ligament should be closely examined to rule out any further deltoid ligament damage and to rule out any probable subtalar injury.
Prevention
Preventative measures include proper warm-up before activities, wearing supportive footwear, and strengthening the muscles around the ankle.
Conclusion
An ankle inversion sprain occurs when the foot rolls inward, overstretching or tearing the ligaments on the outer side of the ankle. Symptoms are Ankle pain, swelling, and difficulty walking.
Treatment typically involves rest, ice, compression, and elevation (RICE), along with physical therapy for recovery. Recovery time can range from a few weeks to several months, depending on the severity of the sprain.

Author: Nitesh Dhameliya
Physiotherapist, Ahmedabad Clinic Name : Samarpan Physiotherapy Clinic Nikol Nava Naroda Branch 11, Vedant Bunglow, Opp. Radhe Bunglow Part -2 Haridarshan Char Rasta, Nikol Naroda Road Behind. Shalby Hospital, near Fortune Circle, Ahmedabad, Gujarat 382330