
Cubitus Varus
Definition for Cubitus Varus
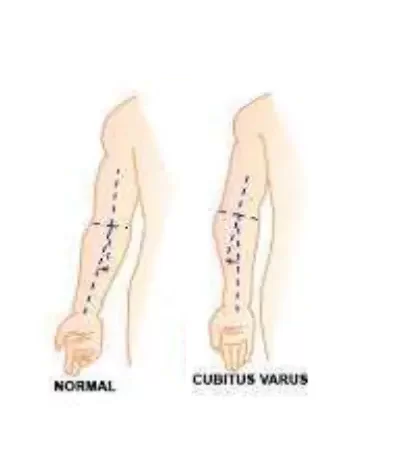
Cubitus varus (varus means a deformity of a limb in which part of it is deviated towards the midline of the body) is a common deformity in which the extended forearm is deviated towards midline of the body.
The “opposite” condition is cubitus valgus.
Malunion of supracondylar fractures often leads to cubitus varus, or “gunstock deformity.” This condition is a triplanar malalignment of the elbow, characterized by varus angulation in the coronal plane, extension in the sagittal plane, and internal rotation in the transverse plane.
INTRODUCTION
Elbow injuries are a frequent occurrence in the skeletally immature pediatric population. The metaphysis of the distal humerus is most susceptible to fractures in this population as it is an area of transition from a tubular configuration to a more flattened triangular cross-section.
In addition to this anatomical peculiarity, ligamentous laxity in this age group predisposes pediatric patients between the age of 4 and 8 years to supracondylar fractures of the humerus. Typically, malunion of supracondylar fractures often leads to cubitus varus, or “gunstock deformity.”
Although it is frequently regarded as a purely cosmetic problem in children, it occasionally causes late-onset lateral elbow pain, symptomatic elbow posterolateral rotatory instability (PLRI), triceps snapping, progressive ulnar and elbow joint varus, ulnar neuropathy, or rarely, predispose to lateral humeral condyle fractures. For this reason, it may be appropriate to offer surgical treatment in the vast majority of patients with this complaint.
Various treatment options proposed include observation, hemiepiphysiodesis and growth alteration, and corrective osteotomy. Corrective osteotomy is the preferred method, as it yields the highest probability for success.

Causes of Cubitus Varus :
Historically, the incidence of this deformity following supracondylar humerus fractures occurred in up to 30% cases. However, the incidence has decreased substantially with the operative, treatment of these injuries. Less commonly, this can occur after lateral condyle humeral fractures. Other causes include physeal injuries, osteonecrosis, infection, or rarely, tumorous conditions.
Patho-Anatomy
The medial deviation of the upper extremity mechanical axis, and the medially directed triceps force vector with this deformity, can ultimately lead to attenuation of the lateral ulnar collateral ligament and ulnar supination, causing symptomatic elbow PLRI. Bone remodeling in the axis of the elbow joint in immature children often restores elbow flexion, although the arc of elbow motion is altered with increased hyperextension and decreased flexion. However, there is little remodeling, and therefore correction, in the rotational component of the deformity. Additionally, these patients can have reduced range-of-motion in pronation.
Internal rotation malunion of the distal humerus leads to several pathoanatomic features such as posterior trochlear, capitellar, and radial head overgrowth. These primary abnormalities lead to secondary adaptive changes, including increased anteroposterior trochlear articular arc and lateral shift of trochlear notch convexity. Furthermore, the ulna adjusts to a distal and medial location with increased varus, flexion, and external rotation. Ulnar nerve instability and delayed ulnar nerve palsy can also occur due to internal rotation malunion of the distal humerus or concomitant fibrosis and entrapment in the cubital tunnel.
The nerve can sublux or even dislocate anterior to the medial humeral epicondyle and becomes entrapped in the fibrous bands of the flexor carpi ulnaris muscle causing symptoms of ulnar nerve neuropathy.
Evaluation
Full-length anterior-posterior radiographs (AP) of the injured and contralateral upper extremity are essential for defining the extent of deformity and estimating the humeral-elbow-wrist angles. The HEW angle provides the most accurate method for determining the correct carrying angle. A HEW angulation is represented with a (+) sign if the extremity alignment is valgus, while a varus angle is denoted with a (-) sign. This approach is used in favor of the Baumann’s angle due to its applicability in both the skeletally immature and adult population.
In the absence of long radiographs, the angle subtended between the center of the shaft to the center of the elbow and the center of the transverse diameter of the radius and ulna provides a reasonable approximation of the HEW angle. The goal of the osteotomies should be the restoration of the HEW angle as close as possible to the contralateral uninjured extremity with the desired correction defined by the difference in the angles between the two extremities. The lateral condylar prominence index is also calculated from the pre-operative AP radiographs of the affected extremity.
The difference between the lateral and the medial width of the distal humerus from the mid humeral axis and is expressed as a percentage of the total width of the distal humerus. True lateral elbow radiographs allow evaluation of the degree of extension deformity that exists. The affected and unaffected extremity radiographs are traced on paper to determine the width of the wedges necessary for surgical correction. A similar technique is employed to determine the required amount of rotation when using the dome osteotomy corrective technique.
The severity of a cubitus varus deformity is graded as follows:
- Grade I – loss of physiologic valgus
- Grade II – varus of 0 to 10 degrees
- Grade III – varus of 11 to 20 degrees
- Grade IV – varus >20 degrees
cubitus varus angle measurement :

PHYSICAL EXAMINATION
A thorough history and physical examination are necessary for the evaluation of a patient with cubitus varus deformity. The presence of open wounds, stiffness, range-of-motion, scarring, and a complete neurovascular examination should take place in the initial visit.
Rotational malalignment is determined by evaluating the differences in shoulder passive internal rotation in extension between the involved uninvolved extremity during physical examination. Progression of deformity in a growing child requires a critical evaluation of radiographs and warrants further axial imaging for assessment of asymmetrical physeal growth abnormalities.
Cubitus varus deformity is commonly recognized 6 to 10 weeks after healing of the fracture and return of complete elbow motion. Varus angulation is mostly responsible for the unsightly appearance of the elbow, while any amount of flexion contracture or posterior angulation reduces the apparent deformity. Torsional malrotation exaggerates the appearance of the deformity. Untreated varus angulation typically remains stable, and rarely if ever, progresses with time.
Progression can occur with asymmetric growth disturbance in the distal humeral physis. If left untreated, or if severe enough, cubitus varus may result in ulnar nerve entrapment and posterolateral rotatory instability from attenuation of the LUCL. Occasionally, PLRI is unmasked after surgical correction.
cubitus varus radiology :
Treatment of Cubitus Varus :
Medical Treatments are mostly symptomatic eg. if pain and swelling around the joint are present then NSAIDS are Prescribed mostly By Doctors.
Physiotherapy Treatment in Cubitus Varus :
Physiotherapy Treatments are Corrective Elbow Mobilization Exercises and Strengthening of Weak Muscles and Stretching of Tight muscles around elbows with Elbow mobilization are prime Goals of Treatment.
Cubitus varus exercises :
- Stretching exercise: After examination, tight muscles around the elbow require proper stretching exercises in a manner to correct the deformity.
- Strengthening Exercise of weak muscles also helps to maintain the normal shape of the elbow and overall correct the deformity
- Elbow Mobilization exercise helps in reducing joint stiffness and also corrects the deformity
Electrotherapeutic techniques like faradism under pressure for correction of deformity, TENS, ULTRASOUND, and PARAFFIN WAX BATH (pain relief and extensibility) where the treatment modalities selected.
Corrective Orthosis / Splints for Cubitus Varus:
Cubitus varus surgery :
Cubitus varus osteotomy :
Corrective osteotomy of the distal humerus is the procedure of choice, as it is most successful in reducing symptoms and recurrence of cubitus varus deformity. The goal of the osteotomy is to correct the alignment of the elbow joint to a normal range of 5 to 15 degrees, as well as create a stable joint. Numerous osteotomy techniques for surgical correction have been described, including straight and oblique lateral closing wedge, reverse V, triangle, dome, double dome, step cut, multiplanar, and external fixation with distraction osteogenesis.
However, no one technique is safer or more successful than others. Besides, it is uncertain whether the correction of axial rotational malunion is necessary to achieve better outcomes, as the carrying angle was not influenced by the degree of uncorrected torsional deformity in one study. This observation is important since attempts at correction through axial derotation often render the osteotomy site unstable from reduced cortical contact. However, the long-term consequences of uncorrected rotational malunion after corrective osteotomy are unknown. Pins, screws, staple, and tension band constructs with wires are typically used for internal fixation of the osteotomy in the pediatric population, as hardware prominence is not uncommon in this age group.
Postoperative Rehabilitation
Postoperative care varies depending upon the corrective procedure undertaken. The posterior above-elbow splint is given for 2 to 3 weeks, followed by active range of motion exercises. The K wires are removed after 4 to 6 weeks depending upon the healing status.
Prognosis:
If untreated, the cubitus varus does not result in functional loss. Cosmetic improvement is the main justification for corrective osteotomy. However, in situations of long-standing deformity with concomitant clinical signs of instability and ulnar neuropathy, surgery is required.
Healthcare Team:
Physiotherapists, radiologists, and paediatric orthopedists work together to treat cubitus varus. The key healthcare professionals are orthopaedic surgeons, and they should be familiar with the often performed corrective osteotomy surgeries. The radiologist aids in a more accurate assessment of deformity factors. The orthopaedics specialty’s nursing staff is extremely crucial. Following surgery, the physiotherapists assist in restoring the range of motion.
FAQ
What is the cubitus varus?
A side effect of a malunited supracondylar fracture is cubitus varus. The varus, hyperextension, and internal rotation components make up the triplanar deformity. The primary reason for surgery is a cosmetic issue, while symptoms of instability and ulnar nerve involvement are other reasons.
What is the cause of cubitus varus?
The cubitus varus, also known as the bow elbow or gunstock deformity, is brought on by malunion, which develops as an aftereffect of a supracondylar humeral fracture. It results in a loss or reduction of the carrying angle in only the extension type of supracondylar fracture of the humerus.
What is the difference between cubitus varus and valgus?
In cubitus valgus deformity the distal part of the forearm deviated laterally while in cubitus varus deformity the distal part of the forearm deviated medially.
What is the treatment for cubitus varus?
The cubitus varus deformity must be surgically corrected to avoid complications such as nerve palsies, subsequent fractures, and lateral instability. In order to repair the deformity, lateral closed wedge osteotomy is a good option. Reduced complications will result from proper stabilization, preferably with a plate and screw.
What nerve is involved in cubitus varus?
In cubitus varus, the ulnar nerve is actively compressed and pulled during elbow flexion by the triceps muscle, causing neuropathy.
Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803




2 Comments