
Extensor Carpi Ulnaris Tendinitis (ECU Tendinitis)
What is a Extensor Carpi Ulnaris Tendinitis?
Extensor carpi ulnaris tendinitis is an injury of the wrist where the extensor carpi ulnaris muscle becomes inflamed and irritated.
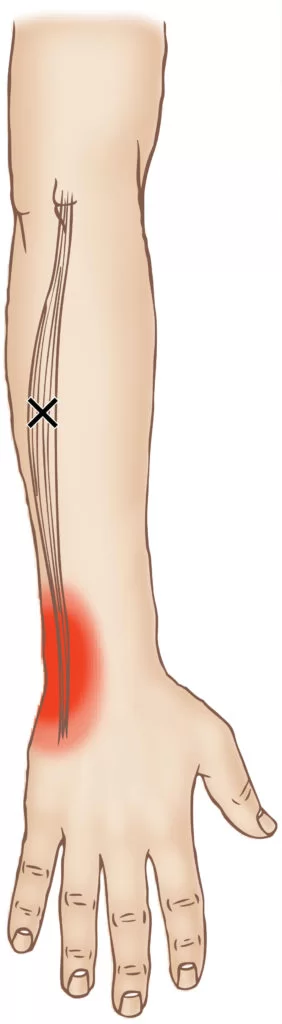
ECU tendinitis is an inflammation of the extensor carpi ulnaris tendon, found on the pinky side of the hand. Symptoms include wrist pain and loss of grip strength. ECU tendinitis symptoms are made worse by combined wrist motion towards the pinky side and moving the palm up and down.
In patients with subluxation of the ECU tendon and disorganisation of the tendon subsheath along the medial side of the head of the ulna, recovery takes two to three months. If the tendon subsheath has not detached, the ECU tendon remains stable and the healing process is more rapid, taking four to six weeks.
Anatomy of Extensor Carpi Ulnaris Muscle
The extensor carpi ulnaris muscle is one of the extensor muscles of the forearm located in the superficial layer of the posterior compartment of the forearm. It shares this compartment with the brachioradialis, the extensor carpi radialis longus, the extensor carpi radialis brevis, the extensor digitorum, and the extensor digiti minimi. All of these muscles share a common origin on the lateral epicondyle via the common extensor tendon. As all of these muscles near their distal insertion sites, they are secured by the extensor retinaculum
Origin
The extensor carpi ulnaris muscle originates from the lateral epicondyle of the distal humerus and the posterior aspect of the ulna.

Insertion
It inserts onto the dorsal base of the fifth metacarpal after passing through the sixth compartment of the extensor retinaculum.
Nerve supply
The muscle receives nerve supply from the posterior interosseous nerve, which is a motor branch of the radial nerve. The radial nerve dives posteriorly through the heads of the supinator muscle in the antecubital fossa to form the posterior interosseous nerve. It innervates the extensor carpi ulnaris muscle in addition to the other muscles in the posterior compartment of the forearm. The radial nerve arises from the brachial plexus by way of the posterior cord which has contributions from the spinal nerve roots of C5 to T1.
Artery
The extensor carpi ulnaris gets its vascular supply primarily from the ulnar artery which branches off of the brachial artery near the antecubital fossa and supplies the medial aspect of the forearm. Due to the muscle’s location in the posterior compartment of the forearm, it also receives some blood supply from the posterior interosseous artery, a posterior branch of the radial artery, that runs between the superficial and deep extensor muscle groups and supplies them both.
Function
The extensor carpi ulnaris serves to extend and adduct the hand at the wrist and also provides medial stability to the wrist. It is a thin muscle which has fibers originating from both the distal humerus, as a part of the common extensor tendon, as well as the proximal ulna.
Clinical Relevance
The extensor carpi ulnaris is an important muscle in the activity of the wrist and forearm that contributes not only to the extension and adduction of the wrist but also to its medial stability. It is most commonly injured in athletes subject to forceful wrist movements. Repetitive flexion and extension of the wrist can lead to tenosynovitis due to the irritation of the tendon and the sheath that holds it in place. Overuse can also lead to tendinopathy of the muscle tendon in which there can be thickening and painful stiffness of the tendon with minimal structural damage. Continued excessive stress on the tendon can cause structural damage which can lead to a partial tear.
Epidemiology
Very common sports overuse syndrome
Mechanism
- Related to racquet sports with repetitive wrist motion
- Squash
- Badminton
- Racquetball
- Rowing
- Tennis
- Tennis player with two handed backhand
- Excessive ulnar deviation in nondominant wrist
Symptoms of Extensor Carpi Ulnaris Tendinitis
The most common symptom of extensor carpi ulnaris tendinitis is pain on the pinky side of the wrist, and this pain usually increases when a person grabs something or bends the wrist toward the pinky side of the hand. Other symptoms of this injury include:
- Swelling
- Stiffness
- Redness
- Decreased range of motion
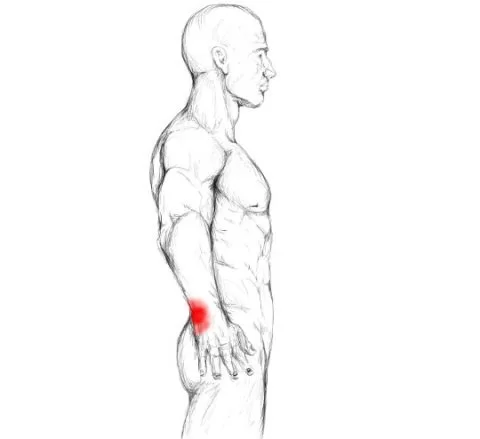
Signs
- Extensor Carpi Ulnaris (ECU) location
- Supination: Dorsal to ulnar styloid
- Pronation: Volar to ulnar styloid
- Tenderness over ECU in sixth dorsal compartment
- Severe pain on resisted supination
Diagnostic procedure
This injury most often requires imaging for a diagnosis. These imaging tests include an MRI or an ultrasound. All three options allow for visualization of the ligamentous tissue of the wrist. Your hand surgeon will perform a physical examination of the wrist and may ask you to flex your hand and extend your wrist to assess limitations in movement and difficulty moving the affected region.
Differential Diagnosis
- Subluxation of ECU (Traumatic rupture of subsheath)
- Thumb Ulnar Collateral Ligament Injury
- Anterior Cubital Tendon Injury
- Pisiform-Triquetrum Joint Injury
- Triquetrum-Lunate Joint Injury
- Triangular Fibrocartilage Complex Injury
Treatment Options for Extensor Carpi Ulnaris Tendinitis
Treatment for extensor carpi ulnaris tendinitis is usually simple, involving rest and treating pain. Mild cases of ECU Tendinitis can be treated with rest, splinting and non-steroidal anti-inflammatories, whereas severe instances can necessitate cortisone injection or surgery to repair the tendon and its sheath which anchors it to the ulna head and wrist (aka subsheath).
Conservative Treatments
Conservative methods include immobilization and stabilization of the affected wrist by placing it in a cast or splint. Some patients may require a long arm fiberglass cast to try to ensure that all wrist movement is completely stopped. Some patients may benefit from a corticosteroid injection to relieve pain and swelling, alongside NSAID pain management.
Surgical Treatments
In the event that this injury does not improve with conservative management, or if the injury is deemed too severe after an initial analysis, surgical intervention may be required. Surgical repair of the ECU is not often required, however, a severe injury may indicate the need for its reconstruction. It is extremely important to see a medical professional at the time of injury or as soon as you know that you have one for the best possible diagnosis.
Preventing Extensor Carpi Ulnaris Tendinitis
Some injuries may be unavoidable, however, utilizing proper body mechanics during athletic activities is extremely important. Additionally, making use of safety equipment during gameplay or wearing a brace on your wrist if it has been injured in the past can help prevent future injury. Players should cease athletic activities at the first sign of pain or discomfort and consult with a medical professional. Often times, allowing the wrist to rest between gameplay and icing the affected region can aide in minimizing long-term wear and tear.
Prognosis for Extensor Carpi Ulnaris Tendinitis
Many patients benefit from a period of rest following an injury to the extensor carpi ulnaris muscle. Your doctor may recommend a period of immobilization for 2-4 weeks following an injury. Surgical intervention may require a healing period of 6-8 weeks, followed by physical therapy. Many patients can look forward to a full recovery with a full range of motion following proper medical intervention and attention to the injury.
Physiotherapy Treatment
Acute tendinosis of the ECU usually responds to non-operative measures of rest with Physiotherapy treatment and exercise, activity modification, splinting (in a position of 30° wrist extension and ulnar deviation), or, occasionally, immobilization in a short-arm plaster cast in the same position for a 3-week period.
Rehabilitation strategies are based on the severity of tendinopathy. Treatment of the early reactive phase consists of load management and isometric exercises until the pain settles (typically over 5–10 days). The load can then be increased in stages. Ibuprofen is thought to be a helpful adjunct during this phase.
In chronic tendinopathy, without a sudden increase in pain, a combination of load management, eccentric work, isometrics, and strength exercises are likely to help.
If symptoms are not relieved by non-operative measures an injection of steroid into the fibro-osseous sheath should be considered.
wrist splint or wrist brace

Modalities
Ice application for initial swelling and pain. TENS for pain relief. A contrast bath might be helpful in reducing pain and swelling.
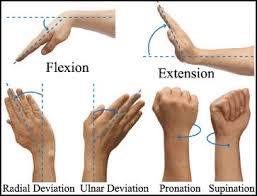
Isometric exercise at the wrist and fingers
Flexion
Hold your forearm steady with the palm up. Use your opposite hand to push against an upward and outward movement of your hand at the wrist.
Extension
Keep your forearm steady in a palm-down position. Use your opposite hand to push against an upward and outward movement of your hand at the wrist.
Radial Deviation
Hold your forearm steady in a thumb-up position. Use your other hand to push against an upward movement at the wrist.
Ulnar Deviation
Hold your forearm steady with the thumb up. Use your other hand to push against a downward movement at the wrist.
Gentle stretching of the wrist and thumb
Starting in the pain-free range can really help. When the wrist and thumb are splinted 24/7 for 6 weeks, the structures can become very tight, so to prevent this your client should remove their splint and gently stretch several times per day (but again, stressing the pain-free range). It is often easier to achieve a comfortable stretch after heat and massage.
Wrist stretch: With one hand, help to bend the opposite wrist down by pressing the back of your hand and holding it down for 15 to 30 seconds. Next, stretch the hand back by pressing the fingers in a backward direction and holding it for 15 to 30 seconds. Keep your elbow straight during this exercise. Do 3 sets on each hand.
Wrist extension stretch: Stand at a table with your palms down, fingers flat, and elbows straight. Lean your body weight forward. Hold this position for 15 seconds. Repeat 3 times.
Wrist flexion stretch: Stand with the back of your hands on a table, palms facing up, fingers pointing toward your body, and elbows straight. Lean away from the table. Hold this position for 15 to 30 seconds. Repeat 3 times.
active assisted exercise of the wrist
Wrist Range of Motion
Flexion: Gently bend your wrist forward. Hold for 5 seconds. Do 3 sets of 10.
Extension: Gently bend your wrist backward. Hold this position 5 seconds. Do 3 sets of 10.
Side to side: Gently move your wrist from side to side (a handshake motion). Hold for 5 seconds at each end. Do 3 sets of 10
Strengthening of wrist and forearm muscles
Strengthening / loading. Soft tissues do not like to be immobilized for long periods. Having the wrist splinted 24/7 may result in weakening and poor organization of the collagen fibres and increased cross-linking between fibres. Isometric loading can very effectively prevent or reverse these effects, and because the loading is isometric it does not cause further friction/irritation of the inflamed soft tissues.
Wrist flexion: Hold a can or hammer handle in your hand with your palm facing up. Bend your wrist upward and outward. Slowly lower the weight and return to the starting position. Do 3 sets of 10. Gradually increase the weight of the can or weight you are holding.
Wrist extension: Hold a soup can or hammer handle in your hand with your palm facing down. Slowly bend your wrist upward and outward. Slowly lower the weight down into the starting position. Do 3 sets of 10. Gradually increase the weight of the object you are holding.
Grip strengthening: Squeeze a rubber ball and hold for 5 seconds. Do 3 sets of 10.


2 Comments