

Modified Ashworth Scale of Spasticity
Modified Ashworth Scale of Spasticity is a common scale to use for measuring spasticity in those with cerebral palsy, stroke, and other neurological disorders. The Modified Ashworth Scale is a scale that is used to quantify the amount of spasticity or stiffness in a patient.
The Modified Ashworth Scale has five different symptom severity levels ranging from 0 to 4. The Modified Ashworth Scale is commonly used to measure spasticity in those with cerebral palsy, stroke, and other neurological disorders.
Used of to the scale :
- It is used to assess the spasticity.
Purpose of the scale :
- It is considered the primary clinical measure of muscle spasticity in patients with neurological conditions.
- It is also a rating scale that measures the abnormality of the tone & the resistance of the passive movements.
In which condition Modified Ashworth Scale of Spasticity is used?
This scale is used in many neurological conditions:
- Stroke
- Spinal cord injury
- Multiple sclerosis
- Cerebral palsy
- Traumatic brain injury
- Pediatric hypertonia
- Central nervous system lesions.
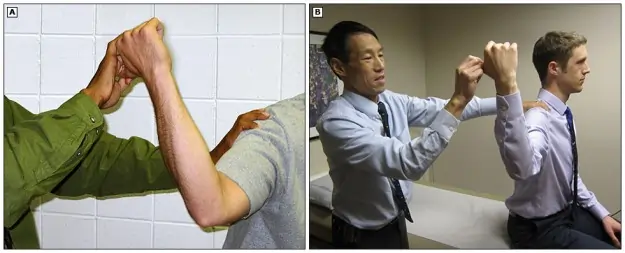
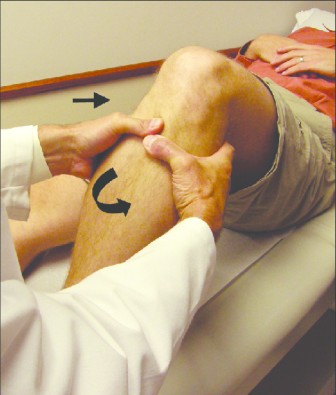
Which is Method Use in this scale?
- Starting position is supine .
- This scale is performed by to the extension of the patients limb .
- First from to the a position of the maximal possible flexion to the maximal possible extension.
- Into Afterwards, this scale is assessed while the move of to the extension to flexion.
What is Equipment need for this scale :
- Training
- Therapy mat
- None typically reported
- Paper
Scoring of Modified Ashworth Scale of Spasticity:
| NO | Description |
| O | Slightly increase into the muscle tone which is giving to a catch when the slightly increase into the muscle tone, which is manifested by the limb, limb is moved into the flexion or extension. |
| 1 | Slightly increase into the muscle tone, which is manifested by the catch followed by the minimal resistance of the throughout (ROM ). |
| 1+ | More marked increase to in muscle tone through to most of the limb but easily for to the flexed . |
| 2 | More marked increase to in muscle tone through to most of to the limb but easily for to the flexed . |
| 3 | Considerable increase into the tone & passive movement is to the difficult |
| 4 | Limb is rigid into the flexion or extension |
Clinical Considerations of this scale :
- This scale is commonly used in the clinical setting which is to the assess the spasticity into the people with to the SCI.
- It is note to the spasticity in the multi-facet & construct with to the individual components of to the spasticity weakly which is related to the each other , it is suggest to the different clinical scales measure to the unique aspects of spasticity.
- It is also measure to the assesses of to the single-joint resistance / passive ROM & velocity dependent stretch reflex.
- It is do not address the spasm frequency or severity .
- It is not to do the differentiate between to the phasic & tonic components of the spasticity.
- So that the overall construct of the spasticity which is the best measured with to the appropriate battery of the tests including this scale .
- This Ashworth or Modified Ashworth both are well-tolerated by the patients.
- This scale is measure easily administered into the during routine clinic visits & does not require the specialized equipment.
Versions of the scale
- This Scale is initially developed in the early 1960s by the Bryan Ashworth.
- In this scale include to the 5-point scale with a grade score of to the 0, 1, 2, 3, or 4 .
- Into the 1987
- Bohannon & Smith are added to the grade – 1 .
- Proposed to the slight changes on to the definitions of to the each score into the order to the increase of the sensitivity to the measure & facilitate the scoring.
- It is called The new measurement of the Modified Ashworth Scale .
- It is considered by the many as the gold standard for to the measuring the spasticity .
Evidence of this scale :
| NO . | Reference | Year | Study details | Relevant results |
| 1 | Bohannon & Smith | 1987 | Inter-rater reliability of to this scale . Tested of muscle : elbow flexors of to the impaired arm. Ns – 30 – include in to the condition of the patient in NS is MS (1), HI (5), CVA (24) . Na – 2 = physiotherapist . Assessors are independently assessed to the each subject of the once. | 86.7% of the agreement between to the assessors means in Kendall’s t = 0.847 & p <0.001 Cohen’s is calculated to the = 0.826a |
| 2 | Bodin and Morris | 1991 | inter-rater reliability of this scale . tested of muscle : elbow flexors & extensors with the knee flexors. Measurements are take to the bilaterally. Ns = 34 – include in to the condition of the patient in Ns is hemiplegia – 34 . Na – 4 = physiotherapist -2 & doctor – 2 . assessors are serially assessed to the each subject . | 76% of to the agreement between to the assessors means in Kendall’s t = 0.857 Cohen’s is calculated to the = 0.745a |
| 3 | Sloan et al. | 1992 | inter-rater reliability of to this scale . tested of muscle : elbow flexors & extensors with the knee flexors. Measurements are take to the bilaterally. Ns = 34 – include in to the condition of the patient in Ns is hemiplegia – 34 . Na – 4 = physiotherapist -2 & doctor – 2 . assessors are serially assessed to the each subject . | Spearman’s is calculated varied from to the 0.56 & 0.90 at to the elbow & between to the 0.26 & 0.62 at to the knee. |
| 4 | Allison et al. | 1996 | Inter & Intra-rater reliability of this scale . Tested of muscle : ankle plantar flexors. Measurements are take to the bilaterally. Day-1 of to the testing = Ns = 30 – include in to the condition of the patient in Ns is HI ; Na – 2 = physiotherapist . Both test are assessed all to the subjects independently. Day-2 of to the testing = Tester 1 ia onle assessed & Ns = 21 subjects. | for to the Day-1 = Inter-rater reliability tester 1 & tester 2 – 55% agreement Include = 0.727; t = 0.647 other is Intra-rater reliability of to the tester 1 is 53% agreement include = 0.741; t = 0.674; Intra-rater reliability of to the tester 2 = 48% agreement include = 0.550; t = 0.478 for to the Day-2 = it is a Intra-rater reliability of to the tester 1: 58% agreement include = 0.821; t = 0.739 |
Reliability of this scale :
- Interrater / Intrarater of the Reliability :
- Use of the muscle tested = Elbow flexor & extensor with to the knee flexor into the Hemiplegia patients.
- Measurements are take to the bilaterally.
- Ns = 34 – include in to the condition of the patient in Ns is hemiplegia = 34
- Na – 4 physiotherapist -2 & doctor – 2.
- The assessors are to the serially assessed to the each subject.
- Spearman’s are calculated to the varied from 0.56 & 0.90 at to the elbow or between to the 0.26 & 0.62 at to the knee .
- Into the daily practice this scale is used to the procedure is to the quick & easy.
- It is a common tool in to the measurement of to the spasticity.
- It is also used as to the in the research, like as to the In different patient groups of to the stroke,multiple sclerosis & spinal cord injury.
- The scale is found to the moderate to good intra-rater reliability & poor to moderate inter-rater reliability .
Validity of this scale :
Criterion Validity :
- in to the 35 patient s see the good correlations between the modified Ashworth scores & EMG parameters which is derived from the simultaneous surface & EMG is recordings to the muscles tested.
- It is not to the possible to the draw unequivocal support of to this scale & being a valid & ordinal measure of to the spasticity due to the one key of the methodological inconsistency.
- Into The actual time of to the grade spasticity is reported to the between 0.25 & 0.33 s but however, many of the derived to the EMG parameters are poorly referenced to the time window.
Construct Validity:
- 13 modified of to the original scale by to the adding an to the additional category,=
- A- 1+ falling is between to the 1 & 2 with to the aim of this increasing the sensitivity.
- Both scales are since been used to the measures of to the spasticity for to the clinical & research purposes.
- Clinical rating of the spasticity on this scale is made after the assessor tests of to the resistance which is provide to the passive movement about the joint.
- Both scales are describe the resistance perceived while the moving a joint through to the full range of movement = except into the grade 4
Content Validity:
- This scale is initially to the developed as to the simple clinical tool to the test which is the efficacy of an to the anti-spastic drug into the patients with to the multiple sclerosis.
Alternative form of this Scale :
Ashworth Scale:
- It is Published into the 1964 .
- This Scale is to the original measurement for to the resistance of the passive movement.
- It is a 5-point of to the scale .
- Which is used with the grade score of the 0, 1, 2, 3, or 4.
- This scale is less sensitive than the Modified Ashworth Scale .
Ashworth Scale Scoring :
| NO | Description |
| 0 | No increase into the muscle tone . |
| 1 | Sightly increase in tone give a catch when the limb was move in flexion / extension . |
| 2 | More marked to the increase in tone but limb is easily to flex . |
| 3 | Considerable increase to the tone so that passive movement is difficult . |
| 4 | Limb is rigid into the flexion / extension . |

2 Comments