
Median Nerve: Anatomy, Origin, Course, Function, Clinical Importance
The Median Nerve is a nerve in humans and other animals in the upper limb. It is one of the five main nerves originating from the brachial plexus.
Anatomy of Median Nerve:
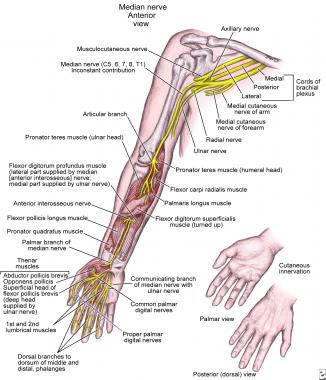
The median nerve originates from the lateral and medial cords of the brachial plexus and has contributions from ventral roots of C5-C7 (lateral cord) and C8 and T1 (medial cord).
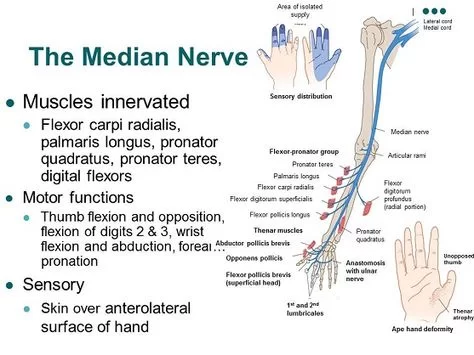
The median nerve is the branch of the brachial plexus that supplies most of the superficial and deep flexors in the forearm, thenar, and lumbrical muscles. It also gives sensation to certain areas of the skin of the hand.
Due to its innervation field, the median nerve enables us to perform both coarse and fine movements of the upper limb, such as opposing our thumb which is important to do precision handling and perform lots of activities like writing, threading a needle, or winding a watch.
Innervation:
The median nerve is a major peripheral nerve and supplies the flexor muscles in the forearm except for flexor carpi ulnaris and the ulnar head of flexor digitorum profundus, which is supplied by the ulnar nerve. It also supplies the thenar muscles as well as the radial two lumbricals.
Median has an interesting sensory supply of the skin in the hand:
- The skin of the palmar and distal dorsal aspects of the lateral three-and-the-half digits and adjacent palm the skin of the palmar and distal dorsal aspects of the thumb and radial half of 2nd digit the skin of palmar and distal dorsal aspects of the adjacent sides of 2nd–4th digits the skin of the central palm.
Origin and nerve roots:
- The nerve roots of the median nerve are from the ventral rami of the C6-T1 nerves.
- The median nerve is formed by the unification of the medial and lateral roots.
- It can be seen as the central line of an ‘M Shaped’ brachial plexus, the cords of which surround the axillary artery.
Course of the Median Nerve:
Arm:
- After its formation from the medial and lateral cords of the brachial plexus, the median nerve descends down the centre of the arm in a superficial course.
- Initially, it is lateral to the brachial artery but as it descends it eventually becomes medial. It gives no branches in the arm.
Forearm:
- Just before it enters the forearm, the median nerve passes between the tendons of the biceps brachii and brachialis. At this point, it becomes lateral to the brachial artery.
- It passes between the deep and superficial heads of the pronator teres muscle. Once it passes this point it dives deeper and runs between the flexor digitorum profundus and superficialis.
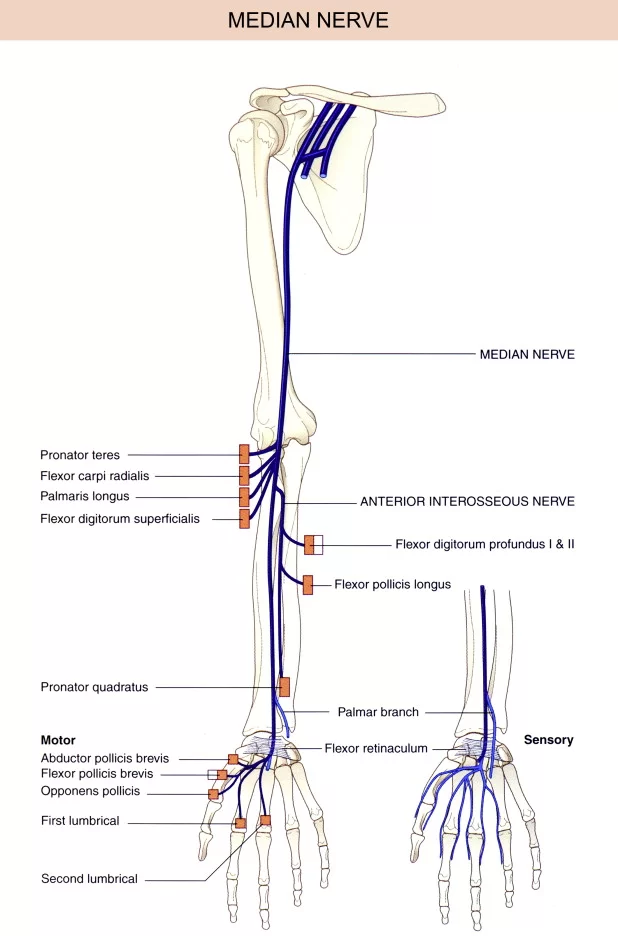
It gives muscular branches:
- Pronator teres
- Palmaris longus
- Flexor digitorum superficialis and flexor carpi radialis
Anterior interosseus nerve
The cutaneous nerve of the palm
- The anterior interosseous nerve supplies the flexor pollicis longus and radial part of flexor digitorum profundus.
- This branch runs on the interosseous membrane with anterior interosseous artery passes deep to the pronator quadratus and supplies it.
- It terminates by giving articular branches to the distal radioulnar, radiocarpal, and carpal joints.
- It also supplies to the proximal part of the palm, via the palmar cutaneous branch.
- This branch does not enter the carpal tunnel and is hence spared in carpal tunnel syndrome.
Hand:
- Median nerve passes through the carpal tunnel beneath the flexor retinaculum, and divides to form two common palmar digital nerves, the first of which supplies the radial two lumbricals and a common branch between the index and middle fingers.
- The second runs between the ring and middle finger, and divides to give the proper digital nerves.
- The branch also provides sensation to the radial three and a half fingers on their palmar aspect as well as the nail beds of the index, middle and half the ring finger, via the proper digital nerves.
The median nerve also gives off a recurrent branch to the muscles of the thenar eminence :
Flexor pollicis brevis, abductor pollicis brevis, opponens pollicis
It is also known as the ‘million dollar nerve’ to signify its importance for basic hand function.
The reason it is referred to as the recurrent branch is due to the course it takes.
- Flexor pollicis brevis, abductor pollicis brevis, opponens pollicis
- It is also known as the ‘million dollar nerve’ to signify its importance for basic hand function.
- The reason it is referred to as the recurrent branch is due to the course it takes.
- It wraps around the flexor pollicis brevis and then arches back to pass into the thenar eminence.
- This does not include adductor pollicis, which although moves the thumb is not a part of the thenar eminence and is supplied by a deep branch of the ulnar nerve.
It wraps around the flexor pollicis brevis and then arches back to pass into the thenar eminence.
This does not include adductor pollicis, which although moves the thumb is not a part of the thenar eminence and is supplied by a deep branch of the ulnar nerve.
Key facts about the median nerve :
Origin: Brachial plexus (C6-T1)
Motor supply: Flexor muscles in the forearm except for flexor carpi ulnaris and the ulnar head of flexor digitorum profundus;
Muscles of the thenar eminence and the radial two lumbricals.
Sensory supply: The skin of the: Palmar and distal dorsal aspects of the lateral three-and-the-half digits and adjacent palm
- Palmar and distal dorsal aspects of the lateral three-and-the-half digits and adjacent palm
- Palmar and distal dorsal aspects of the thumb and radial half of 2nd digit
- Palmar and distal dorsal aspects of the adjacent sides of the 2nd–4th digits
- Central palm
Clinical relations: Carpal tunnel syndrome, a hand of Benediction, simian/ape hand deformity, pronator syndrome
Variation of Median nerve:
The naturally occurring anomalies of the median nerve are:
- Bifurcation of the median nerve typically occurs after the nerve exits the carpal tunnel, in a small percentage (5-10%) of individuals, the median nerve bifurcates more proximal in the carpal tunnel, wrist, or forearm.
- During gestation, a median artery that serves the hand retracts. However, in some individuals, the median artery does not retract and follows the course next to the median nerve into the hand.
- Martin-Gruber anastomoses can occur when branches of the median nerve cross-over in the forearm and merge with the ulnar nerve to innervate portions of the forehand.
- Riche-Cannieu anastomoses can occur when a connection exists between a recurrent branch of the median nerve and a deep branch of the ulnar nerve of the hand.
Function of Median nerve:
The median nerve is the main nerve in the front of the forearm. It supplies the muscles of the front of the forearm and muscles of the thenar eminence, thus controlling the coarse movements of the hand. Therefore, it is also called “labourer’s nerve”.
Arm
- The median nerve has no voluntary motor or cutaneous function in the brachium. It gives vascular branches to the wall of the brachial artery. These vascular branches carry sympathetic fibers.
Forearm
- It innervates all of the flexors in the forearm except flexor carpi ulnaris and that part of flexor digitorum profundus that supplies the fourth and fifth digits. The latter two muscles are supplied by the ulnar nerve (specifically the muscular branches of the ulnar nerve).
The main portion of the median nerve supplies these muscles:
Superficial group:
- Pronator teres
- Flexor carpi radialis
- Palmaris longus
Intermediate group
- Flexor digitorum superficialis muscle
- The anterior interosseus branch of the median nerve supplies these muscles:
Deep group:
- Flexor digitorum profundus (only the lateral half)
- Flexor pollicis longus
- Pronator quadratus
Hand
- In the hand, the median nerve supplies motor innervation to the first and second lumbrical muscles.
- It also supplies the muscles of the thenar eminence by a recurrent thenar branch.
- The rest of the intrinsic muscles of the hand are supplied by the ulnar nerve.
- The median nerve innervates the skin of the palmar (volar) side of the index finger, thumb, middle finger, half the ring finger, and nail bed.
- The radial aspect of the palm is supplied by the palmar cutaneous branch of the median nerve, which leaves the nerve proximal to the wrist creases.
- This palmar cutaneous branch travels in a separate fascial groove adjacent to the flexor carpi radialis and then superficial to the flexor retinaculum. It is, therefore, spared in carpal tunnel syndrome.
Clinical Importance of Median Nerve:

- Carpal Tunnel Syndrome:
- Compression of the median nerve within the carpal tunnel can cause carpal tunnel syndrome (CTS).
- It is the most common mononeuropathy and is caused by increased tissue pressure within the carpal tunnel. Whilst risk factors for CTS have been identified (such as diabetes, pregnancy, and acromegaly), the exact underlying etiology is not well understood.
- Clinical features include numbness, tingling, and pain in the distribution of the median nerve. Importantly, the palm is usually spared – as the palmar cutaneous branch does not travel through the carpal tunnel. Symptoms can wake the patient from sleep and are usually worse in the morning. If left untreated, chronic CTS can cause weakness and atrophy of the thenar muscles.
Tests for carpal tunnel syndrome can be performed during physical examination:
Tinel’s sign–
- Tapping the nerve in the carpal tunnel to elicit pain in the median nerve distribution.
- Phalen’s maneuver – holding the wrist in flexion for 60 seconds to elicit numbness/pain in the median nerve distribution.
- Treatment involves the use of a splint, holding the wrist in dorsiflexion overnight to relieve symptoms. If this is unsuccessful, corticosteroid injections into the carpal tunnel can be used. In severe cases, surgical decompression of the carpal tunnel may be required.
Lesions of the Median Nerve:
Damaged at the Elbow:
Mechanism of injury: Supracondylar fracture of the humerus.
Motor functions:
- The flexors and pronators in the forearm are paralyzed, with the exception of the flexor carpi ulnaris and the medial half of the flexor digitorum profundus.
- The forearm is constantly supinated, and wrist flexion is weak (often accompanied by adduction, because of the pull of the flexor carpi ulnaris).
- Flexion at the thumb is also prevented, as both the longus and brevis muscles are paralyzed.
- The lateral two lumbrical are affected, and the patient will not be able to flex at the MCP joints or extend at IP joints of the index and middle fingers.
Sensory functions:
Lack of sensation over the areas that the median nerve innervates.
Characteristic signs:
The thenar eminence is wasted, due to atrophy of the thenar muscles. If the patient tries to make a fist, only the little ring fingers can flex completely. This results in a characteristic shape of the hand, known as the hand of benediction.
Damaged at the Wrist :
Mechanism of injury:
Lacerations are just proximal to the flexor retinaculum.
Motor functions:
- Thenar muscles are paralyzed, as are the lateral two lumbricals. This affects the opposition of the thumb and flexion of the index and middle fingers.
Sensory functions:
Same as an injury at the elbow.
Characteristic signs:
The hand is held in the same position as damage at the elbow, but the forearm is unaffected (not supinated or adducted, wrist flexion is likely unaffected, depending on the location of the lesion).

20 Comments