

Wrist ganglion and physiotherapy management
- A ganglion cyst or a Bible cyst is a benign swelling or bulge that often appears around or on joints and tendons in the hand or foot. A ganglion manifests as a subcutaneous lump or nodule. The size can change in time and it can also disappear completely.
- In most cases, ganglion cysts are painful, especially in the beginning. But pain severity is not related to the size of ganglions. A ganglion in the musculoskeletal system is a spherical accumulation of fluid production from an adjacent joint capsule or tendon sheath.
- A ganglion cyst is not a cyst because the collection of clear viscous fluid is contained in a cavity, which is not lined by epithelium.
- A ganglion cyst is most frequently located around the dorsum of the wrist and the fingers. Along the musculus extensor carpi radialis brevis is a common site of occurrence because it passes over the dorsum of the wrist joint. In the wrist, they are found especially at the scapholunate area.
Etiology of Wrist ganglion
- Ganglion cysts are the most common soft tissue tumors of the hand and wrist Ganglion is mucin-filled hernia of synovial tissues form joint capsules or tendon sheaths due to one way valve phenomenon.
- The cyst expand in size and the fluid cannot flow freely back into the synovial cavity. A ganglion cyst usually appear spontaneously without any particular cause. Anyone can be affected by ganglion cysts, but they occur 3 times as often in women as they do in men.
- The occurrence of a ganglion cyst is related with osteoarthritis, and therefore most commonly seen in older patients. Ganglion cysts are predominantly seen in young adults and are rare in children.
- The etiology of the ganglion cyst is unclear, although prior trauma, synovial herniation, internal derangement, and a degenerative process associated with mucin production are possible. Wrist ganglion cysts may connect to an adjacent joint in up to 70% of cases and are more common by women
- The degeneration of the connective tissue may be caused by an irritation or chronic damage causing the mesenchyml cells or fibroblasts to produce mucin.

Clinical features of Wrist ganglion
- Ganglions are tumors that present adjacent to joints or tendons. The most common sites for ganglions are the dorsal aspect of the wrist near the scapholunate (SL) joint, the volar wrist near the radioscaphoid joint or the pisotriquetral joint, and the volar retinaculum between the A1 and A2 pulleys.
- Ganglions are usually minimally symptomatic. However, depending on the location of the cyst, patients may present with a myriad of symptoms such as dull aching pain, change in size, spontaneous drainage, and sensory nerve dysfunction.
Diagnosis of Wrist ganglion
- Ultrasound was used to confirm the diagnosis of a ganglion cyst and provide guidance for needle aspiration, fenestration, and subsequent steroid-anesthetic mixture injection. Other methods that are being used are MRI scans.
- This depends on where the ganglion cyst is located. Using magnetic resonance imaging is essential for the differential diagnosis, such as other masses like vascular lesions and lipomas.
- Another diagnostic tool in the evaluation of a ganglion cyst is the use of a radiopaque contrast dye.
- Gangliography is a method of evaluating the size and extent of a ganglion cyst and is performed as an adjunct to aspiration. After the injection of a few. milliliters of contrast dye, a radiograph is obtained, and the extent of the lesion is more easily visualized.
Examination of Wrist ganglion

- The diagnosis ganglion cyst can be made by the physician on the basis of a clinical trial or based on history. If we think wear or trauma is the cause, we introduce some additional investigations: ultrasound, X-ray, or an MRI. These studies are not painful.
- These results are given by a standard of intra-operative determination of the disease. The MRI is performed when atypical features or neurologic symptoms are present and in specific preoperative settings.
- On MRI a cyst has a low signal intensity compared with muscle. Ultrasound is often sufficient for assessing typical cysts. It may be done to detect the presence of occult cysts.
- To exclude any more serious underlying pathology, radiographs in anteroposterior and lateral views are obtained. On ultrasound, a simple cyst is well circumscribed and anechoic with posterior acoustic enhancement.
- The plastic surgeon will also conduct research into the physical of existence of a possible trigger finger. Physicians can often make a diagnosis on the basis of the phenomena. These phenomena are a subcutaneous lump, lump, or nodule of that size that can change. It is usually a soft bulge like the size of a pea.
- In the beginning, ganglion cysts are painful. Besides pain, ganglion-limiting movement causes loss of strength, mostly due to pressure from the swelling on adjacent tendons or nerves. In most cases, additional studies may be omitted.
Medical management of Wrist ganglion
- Many ganglion cysts can disappear without any treatment at all. Various treatments have been proposed over the years. Some include telling people with cysts without symptoms not to worry, using a needle to remove the cyst’s contents (aspiration), or surgery.
- Aspiration usually includes placing a needle into the cyst, drawing the liquid material out, and injecting a steroid compound into the empty cavity (which acts as an anti-inflammatory agent).
- Aspiration is a beneficial and simple option for acute management but appears to have a little long-term impact on resolution. Aspiration appears to be significantly more successful in ganglia of the flexor tendon sheath of the hand with success up to 60% or 70% of the time.
- Surgical excision remains the gold standard for the treatment of ganglion cysts, the surgical techniques include the excision of the entire ganglion complex, including the cyst, pedicle, and a cuff of the adjacent joint capsule. After the surgery, the wrist is sometimes getting a splint to keep it from moving.
- It is to prevent the wrist motion from pumping synovial fluid through the one-way valve mechanism and refilling the cyst. This has proven no more effective than simple aspiration and in postoperative patients leads to prolonged joint stiffness and decreased range of motion. Most studies, even with repeat aspirations, demonstrate a success rate of only 30-50%.
- If you compare aspiration/injection and surgical removal, in general, cysts return less often after surgery. A higher recurrence rate is found in patients with a longer history, larger ganglia, and less experienced surgeons. The ganglion location, age, and gender have no influence on the recurrence rate.
PHYSIOTHERAPY MANAGEMENT
- A ganglion cyst can have consequences for daily activities. Surgical excision is not always done, sometimes the cyst can disappear without any treatment at all or with therapy alone.
- The therapy is aimed at the normal use of the hand. If therapy is given after surgical excision then the accent is on exercise, splint therapy, edema relief, and scar tissue reduction.
- As pointed out above the main goal of physical therapy is to restore the normal use of the hand. Therefore we need to regain full mobility of all the joints of the hand. In most protocols following exercises are used to achieve full mobility
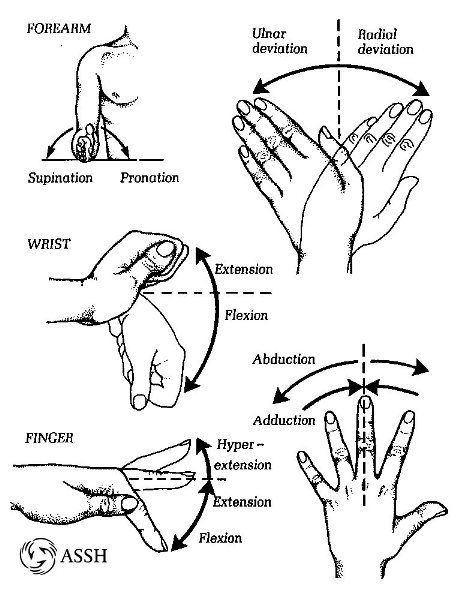
- ACTIVE RANGE OF MOTION EXERCISE: there are 3 finger joints (MCP, PIP, and DIP-joints) and 2 wrist joints (radiocarpal en mediocarpal joint). It’s important that all the possible movements are trained.
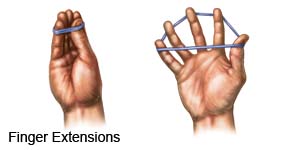
- RESISTED EXERCISE: the resisted exercise of MCP, PIP, and DIP joints will improve the strength of the muscle.
- PNF (proprioceptive neuromuscular facilitation) exercises: the finger is kept in flexion by the therapist. The patient needs to keep this position for a while (active), afterwards the patient relaxes the finger. Repeat for all fingers.
- Tendon gliding exercises: from wrist flexion with finger extension to wrist extension with finger flexion.
- Blocking exercises: lay your hand palm side up on a table. With your opposite hand grasp and hold the affected finger at the middle section just below the end joint. Bend and straighten the finger at the end joint only while holding the rest of the finger straight. Repeat for all joints and fingers.
- It’s also important to reduce scar tissue to restore functional mobility, improve range of motion, and decrease pain. Scar tissue remodeling occurs as you start to stretch and pull on it. Stretching of, in this case, the hand helps to align the collagen fibers to allow them to return to normal.
- This realignment of the collagen fibers makes the tissue better able to tolerate the forces that are placed on it during the day. Another way to help remodel scar tissue in the skin is massage. This can also help loosen any adhesions between the scar, underlying tissue, and fascia. Stretching, and scar massage along with flexibility and strength exercises can help loosen the scar tissue and ensure that proper remodeling takes place.
other related posts :




One Comment