
Trigger finger and Physiotherapy Management
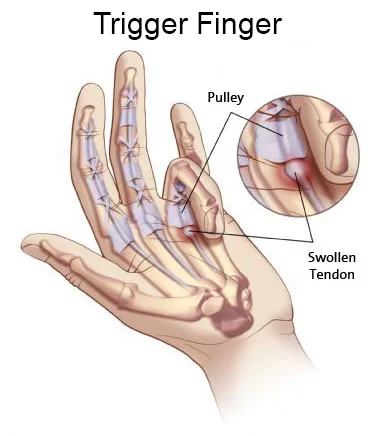
- Trigger finger is a “snapping” or “locking” condition of any of the digits of the hand when opening or closing. Stenosing tenosynovitis is the medical term for trigger finger.
Anatomy related to Trigger finger
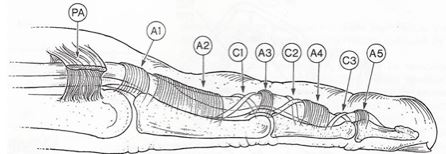
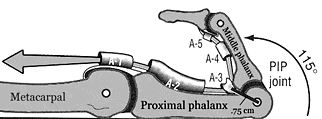
- Each digit of the hand has the ability to move freely throughout a full ROM into flexion and extension. The efficiency, fluidity, and forcefulness of such movement are made possible by several “pulleys” along each digit of the hand. These pulley systems are comprised of a series of retinacular-type structures that are either annular or cruciform in nature. There are five annular pulleys (A1-A5) and three cruciform pulleys (C1-C3).
- The Flexor Sheath and Pulley System
- The flexor sheath and pulley system of the digits ensures the flexor tendons remain in the joint’s axis of motion and prevents bowstringing.
There are three types of pulleys involved:
- Palmar aponeurosis – arises from the palmar aponeurosis and is made up of transverse fascicular bands.
- Annular ligaments (5 in total) – A2 and A4 prevent bowstringing; A1, A3, A5 overlie the Metacarpophalangeal (MP), Proximal Interphalangeal (PIP), and Distal Interphalangeal (DIP) joints respectively.
- Cruciate ligaments (3 in total) – prevent collapsing and expansion of the sheath during movement of the digits.
Pathophysiology of Trigger finger
- Trigger finger is thought to be caused by inflamation and subsequent narrowing of the A1 pulley of the affected digit, typically the third or fourth.
- A difference in size between the flexor tendon sheath and the flexor tendons may lead to abnormalities of the gliding mechanism by causing actual abrasion between the two surfaces, resulting in the development of progressive inflamation between the tendons and the sheath.
Symptoms of Trigger finger
- Finger stiffness, particularly in the morning
- A popping or clicking sensation as you move your finger
- Tenderness or a bump (nodule) in the palm at the base of the affected finger
- Finger catching or locking in a bent position, which suddenly pops straight
- Finger locked in a bent position, which you are unable to straighten
- The trigger finger can affect any finger, including the thumb. More than one finger may be affected at a time, and both hands might be involved. Triggering is usually more pronounced in the morning, while firmly grasping an object or when straightening your finger.
- Trigger finger has a range of clinical presentations. Initially, patients may present with painless clicking with the movement of the digit that can progress to painful catching or popping, typically at the MCP or PIP joints.
- Possible additional symptoms are stiffness and swelling (especially in the morning), loss of full flexion/extension, palpable painful nodule, and/or finger locked into a flexed position. Other signs and symptoms are slight thickenings at the base of the digit and pain that may radiate to the palm or to the distal aspect of the digit.
Examination
History
- Recent trauma
- Job-related repetitive movements
- Locking or snapping while flexing or extending the affected digit
- Radiating pain to the palm or digits
- Past Medical History
- Diabetic individuals are 4x more likely to develop trigger finger
- Disorders causing connective tissue changes such as RA and Gout
Observation
- A digit locked in-flexion
- Bony proliferative changes in the sub adjacent PIP joint
Palpation
- Painful nodule in the palmar MCP secondary to intra-tendinous swelling.
Range of Motion
- Loss of motion, particularly in extension
- Manual Muscle Testing
- Flexor Digitorum Profundus
- Flexor Digitorum Superficialis
- Grip strength using the Jamar Dynameter
- Note: If the finger is locked, testing may not be possible.
Joint Accessory Mobility
- PIP, MCP, DIP, and CMC of all affected digits
- Surrounding tissues
- Wrist joint
- Special Tests
- Open and Close hand
Treatment of Trigger finger
- Trigger finger treatment varies depending on its severity and duration.
Medications
- Nonsteroidal anti-inflammatory drugs — such as ibuprofen or naproxen — may relieve the pain but are unlikely to relieve the swelling constricting the tendon sheath or trapping the tendon.
- The chronic nature of the symptoms associated with the trigger finger makes conservative treatment difficult and often frustrating. Still, conservative care is always recommended as a treatment plan prior to surgical intervention.
Medical Management
- Corticosteroid use has been shown to be effective in reducing pain and frequency of triggering. The shot is injected into the affected tendon and reduces the inflammation and pressure on the tendon for better gliding through the flexor pulleys.
- Application by a primary care provider is an effective and safe alternative to surgical therapy. Patient satisfaction, safety, and functional improvement are characteristics of steroidal injections in comparison to surgical treatment. Surgery is associated with higher costs, long absence from work, and the possibility of surgical complications.
- Studies have also shown the combination of corticosteroid injections with lidocaine to have significantly more effective than lidocaine alone. However, symptoms have shown to return longterm (4-6 months) when treated with injections only.
Open Surgical Technique
- This technique, considered to be the gold standard, is performed by making a longitudinal incision in the palmar crease over the metacarpophalangeal joint of the involved digit and followed by the release of the flexor digitorum superficialis and profundus tendons.
- This procedure lasts 2-7 minutes and has a longer average time of discomfort (45 days) post-op.
- An advantage of this technique is it allows the pulley to be visualized and therefore has less risk of damage to the digital nerves compared to endoscopic techniques.
Endoscopic Surgical Technique
- This technique is performed by making two incisions: one at the palmar crease over the metacarpophalangeal and the other at the volar crease of the finger.
- An endoscope is then introduced to cut the pulley releasing the flexor tendons. This procedure lasts 2-9 minutes and has a shorter average time of discomfort (23 days) post-op.
- Other advantages are the absence of scars and scar-related problems and shorter post-op rehabilitation. However, there is a large learning curve and the instruments are costly.
PERCUTANEOUS RELEASE
- This technique can be performed with or without imaging. Non-image-guided (blind) percutaneous release is performed by using anatomical landmarks to avoid injury to the tendons and neurovascular structures.
- The recovery time is shorter than open surgery but the chance for damage to digital nerves is higher, especially to digits 1, 2, and 5.
- A new technique using ultrasound-guidance helps clearly identify the tendons and neurovascular structures, preventing potential complications that are present with non-image-guided percutaneous release and it also compares favorably with surgical techniques.
Physio Therapy Management of Trigger finger
- As with all disorders of the upper extremity, proximal segments must be screened. Also, because posture can contribute to distal problems, it should be addressed to provide the patient with optimal outcomes.
- HOT PACK – Heat can help relax and loosen tight musculature, improves the blood circulation.
- ICE PACK –ice can be used to help relieve inflammation of the extensor sheath.
- ULTRASOUND THERAPY: UltraSound is therapeutic modalities that generate ultrasound causes deep heat, provide micro-massage to soft tissue, increase flexibility, promote healing of tissue as well improve localized blood supply to the area. and ultimately pain relief electric stimulation, massage, stretching, and joint motion (active and passive) can have some positive effects on the trigger finger. It is thought that heat can help by providing increased blood flow and extensibility to the tendon.
- The following heat with stretching can provide more extensibility with plastic deformation. Joint movement and mobilizations increase joint and soft tissue mobility via a slow, passive therapeutic traction and translational gliding
Patient Education in Trigger finger
- Since the trigger finger is observed as an overuse injury, education is very important. Education should be given on:
- Rest
- Modifications of activities
- Specialized tools
- Splinting
- Modalities
- Posture
- Splinting
- The first step in treatment is to stop doing activities that aggravate the condition. Splinting is one of the best ways to limit motion.. Splints are usually worn for 6-10 weeks. It should be noted that splinting yields lower success rates in patients with severe triggering or longstanding duration of symptoms.
Two major types of splinting

- Splinting at the DIP joint. This showed to have a resolution in 50% of the patient’s symptoms.
- Splinting at the MCP joint with 15 degrees of flexion.
- MCP Splints MCP Splint on Hand
you should read these :

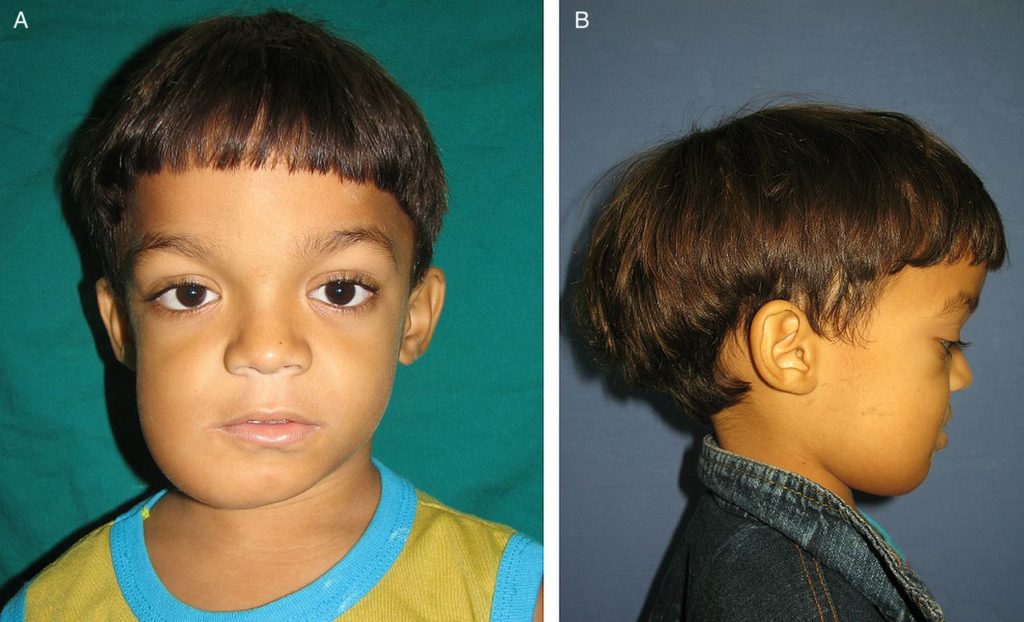
Infantile Osteopetrosis

Author: Bhoomi Physiotherapist
Bhoomi Patel - Physiotherapist in Mobile Physiotheray Clinic, B - 01, Jagatnagar Society, Opp. Shaktidhara Society, India Colony Road, Tollnaka, Bapunagar, Ahmedabad.


6 Comments