Gluteal Nerve: Anatomy, Function, Importance
Gluteal nerve divides in superior & inferior gluteal nerve
1.Superior gluteal nerve
2.Inferior gluteal nerve
1.Superior gluteal nerve
Anatomy of Superior Gluteal Nerve:
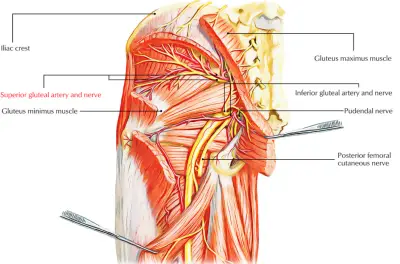
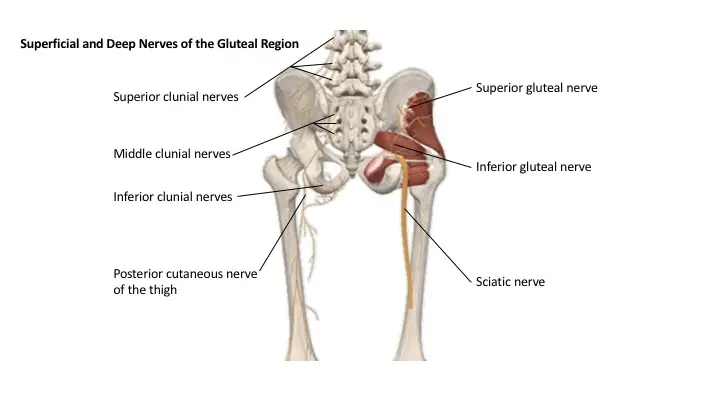
The superior gluteal nerve (L4, L5, S1) passes through the sciatic notch above the piriformis muscle.
It supplies the gluteus medius, minimus, and tensor fasciae latae muscles. The inferior gluteal nerve (L5, S1, S2) supplies the gluteus maximus.
Origin:
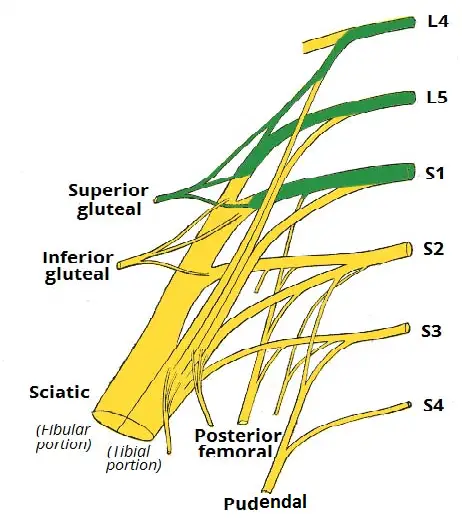
The superior gluteal nerve arises from the posterior divisions of the sacral plexus along with the sciatic nerve, inferior gluteal nerve, and coccygeal plexus.
It is formed from the L4-S1 nerve roots and shortly after forming exits the pelvis through the greater sciatic foramen.
Of all the nerves that exit through the greater sciatic foramen, the superior gluteal nerve is the only nerve to pass above the piriformis muscle.
Course:
After exiting the pelvis the superior gluteal nerve enters the gluteal region and spirals up over the inferior border of the gluteus minimus muscle.
The nerve then travels anteriorly and laterally in a plane between the gluteus medius and gluteus minimus muscles.
Branches:
The superior gluteal nerve ramifies between the gluteal minimus and maximus muscles and distributes branches to both of these muscles.
The superior gluteal nerve terminates by piercing and innervating the tensor fasciae latae muscle.
Relations:
The superior gluteal nerve is the only nerve that departs the pelvis through the greater sciatic foramen above the piriformis muscle. It is accompanied by the superior gluteal artery and vein.
The other nerves that exit through the greater sciatic foramen, including the pudendal nerve, inferior gluteal nerve, and sciatic nerve, exit below the piriformis muscle.
Structure and Function of Superior Gluteal Nerve:
- The superior gluteal nerve provides innervation to the gluteus medius, gluteus minimus, and tensor fasciae latae muscles.
- The gluteus medius muscle is responsible for hip joint abduction and works in conjunction with the gluteus minimus and tensor fasciae latae.
- The gluteus minimus not only allows for hip abduction but is also integral to the medial rotation of the thigh due to its anterior component.
- The tensor fasciae latae, on the other hand, provides traction on the iliotibial tract, thereby assisting in hip extension via the gluteus maximus muscle.
- Together, all three components comprise the abductor mechanism, which stabilizes the pelvis during the single-leg phase of gait while enabling foot clearance during the swing phase.
- The superior gluteal nerve originates from the posterior divisions of the L4, L5, and S1 nerve roots of the sacral plexus, and accompanies the inferior gluteal nerve, sciatic nerve, and coccygeal plexus.
- The nerve then travels posterolaterally, eventually leaving the pelvis through the greater sciatic foramen accompanied by the superior gluteal vessels.
- The superior gluteal nerve is unique in that it is the only nerve to exit through the greater sciatic foramen superior to the piriformis muscle.
- All other nerves that exit through the greater sciatic foramen, such as the pudendal nerve, inferior gluteal nerve, and sciatic nerve, do so inferior to the piriformis.
- It then enters the gluteal region and travels over the inferior aspect of the gluteus minimus, then courses anteriorly and laterally within the plane between the gluteus minimus and gluteus medius muscles, with branches terminating in the tensor fasciae latae muscle.
- Superior to the piriformis muscle the superior gluteal nerve divides into its superior branch and inferior branch.
- The superior division travels with the upper component of the deep division of the superior gluteal artery and innervates the gluteus medius and occasionally the gluteus minimus as well.
- The superior gluteal nerve courses across the deep aspect of the gluteus medius at an estimated 5cm above the tip of the greater trochanter.
- The inferior branch of the superior gluteal nerve, on the other hand, accompanies the lower portion of the deep division of the superior gluteal artery, and travels across the gluteus minimus, innervating this muscle as well as the gluteus medius.
- The inferior branch eventually terminates in and innervates the tensor fasciae latae muscle.
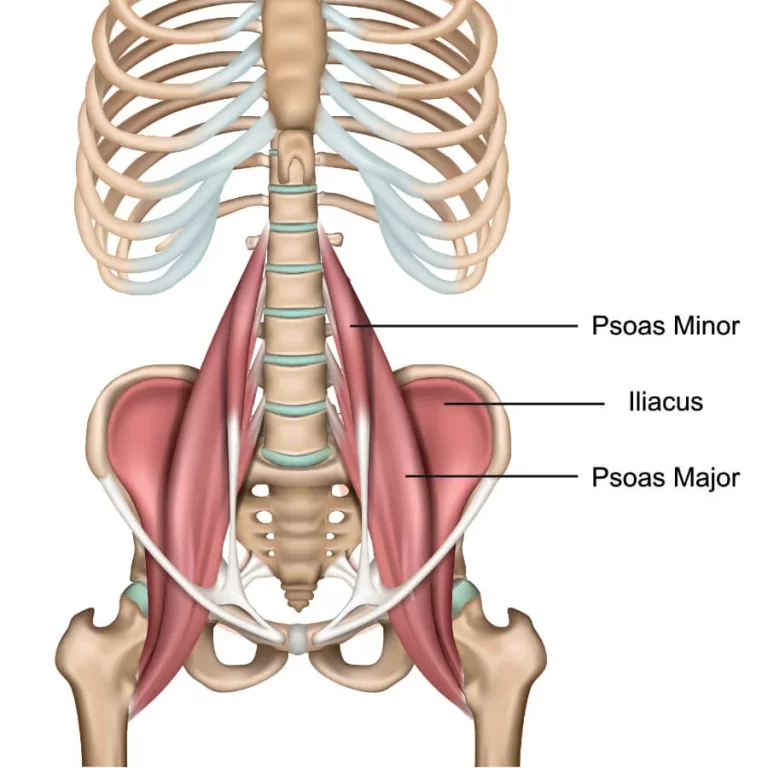
The Superficial Muscles:
The superficial muscles in the gluteal region consist of the three glutei and the tensor fascia lata. They mainly act to abduct and extend the lower limb at the hip joint.
Gluteus Maximus:
- The gluteus maximus is the largest of the gluteal muscles. It is also the most superficial, producing the shape of the buttocks.
- Attachments: Originates from the gluteal (posterior) surface of the ilium, sacrum, and coccyx. It slopes across the buttock at a 45-degree angle and then inserts into the iliotibial tract and the gluteal tuberosity of the femur.
- Actions: It is the main extensor of the thigh, and assists with lateral rotation. However, it is only used when force is required, such as running or climbing.
- Innervation: Inferior gluteal nerve.
Gluteus Medius:
- The gluteus medius muscle is fan-shaped and lies between to the gluteus maximus and the minimus. It is similar in shape and function to the gluteus minimus.
- Attachments: Originates from the gluteal surface of the ilium and inserts into the lateral surface of the greater trochanter.
- Actions: Abducts and medially rotates the lower limb. During locomotion, it secures the pelvis, preventing pelvic drop of the opposite limb. (Note: the posterior fibres of the gluteus medius are also thought to produce a small amount of lateral rotation).
- Innervation: Superior gluteal nerve.
Gluteus Minimus:
- The gluteus minimus is the deepest and smallest of the superficial gluteal muscles. It is similar in shape and function to the gluteus medius.
- Attachments: Originates from the ilium and converges to form a tendon, inserting to the anterior side of the greater trochanter.
- Actions: Abducts and medially rotates the lower limb. During locomotion, it secures the pelvis, preventing pelvic drop of the opposite limb.
- Innervation: Superior gluteal nerve.
Tensor Fascia Lata:
- Tensor fasciae lata is a small superficial muscle that lies towards the anterior edge of the iliac crest. It functions to tighten the fascia lata, and so abducts and medially rotates the lower limb.
- Attachments: Originates from the anterior iliac crest, attaching to the anterior superior iliac spine (ASIS). It inserts into the iliotibial tract, which itself attaches to the lateral condyle of the tibia.
- Actions: Assists the gluteus medius and minimus in abduction and medial rotation of the lower limb. It also plays a supportive role in the gait cycle.
- Innervation: Superior gluteal nerve
The Deep Gluteal Muscles:
- The deep gluteal muscles are a set of smaller muscles, located underneath the gluteus minimus.
- The general action of these muscles is to laterally rotate the lower limb. They also stabilize the hip joint by ‘pulling’ the femoral head into the acetabulum of the pelvis.
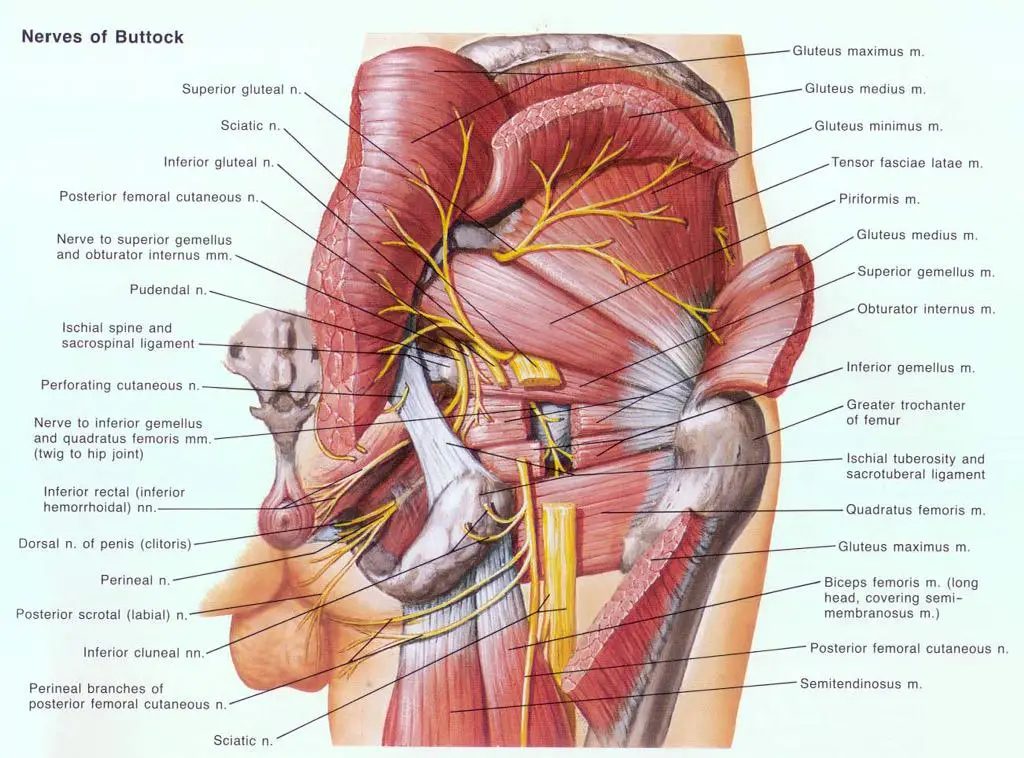
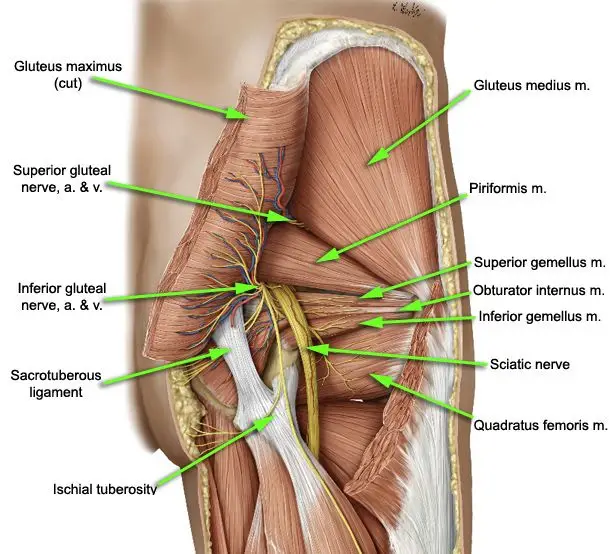
Piriformis:
- The piriformis muscle is a key landmark in the gluteal region. It is the most superior of the deep muscles.
- Attachments: Originates from the anterior surface of the sacrum. It then travels infero-laterally, through the greater sciatic foramen, to insert into the greater trochanter of the femur.
- Actions: Lateral rotation and abduction.
- Innervation: Nerve to piriformis.
Obturator Internus:
- The obturator internus forms the lateral walls of the pelvic cavity. In some texts, the obturator internus and the gemelli muscles are considered as one muscle – the triceps coxae.
- Attachments: Originates from the pubis and ischium at the obturator foramen. It travels through the lesser sciatic foramen, and attaches to the greater trochanter of the femur.
- Actions: Lateral rotation and abduction.
- Innervation: Nerve to obturator internus.
The Gemelli – Superior and Inferior:
- The gemelli are two narrow and triangular muscles. They are separated by the obturator internus tendon.
- Attachments: The superior gemellus muscle originates from the ischial spine, the inferior from the ischial tuberosity. They both attach to the greater trochanter of the femur.
- Actions: Lateral rotation and abduction.
- Innervation: The superior gemellus muscle is innervated by the nerve to obturator internus, the inferior gemellus is innervated by the nerve to quadratus femoris.
Quadratus Femoris:
- The quadratus femoris is a flat, square-shaped muscle. It is the most inferior of the deep gluteal muscles, located below the gemelli and obturator internus.
- Attachments: It originates from the lateral side of the ischial tuberosity, and attaches to the quadrate tuberosity on the intertrochanteric crest.
- Actions: Lateral rotation.
- Innervation: Nerve to quadratus femoris
Clinical Relevance: Damage to the Superior Gluteal Nerve
- The superior gluteal nerve innervates the gluteus medius and the gluteus minimus. These muscles have an important role in stabilizing the pelvis during locomotion.
- In the standing position, the gluteus minimus and medius contract when the contralateral leg is raised, preventing the pelvis from dropping on that side.
- If the superior gluteal nerve is damaged, the previously described muscles are paralyzed – and the pelvis becomes unsteady. A characteristic finding of gluteal muscle weakness is the Trendelenburg sign.
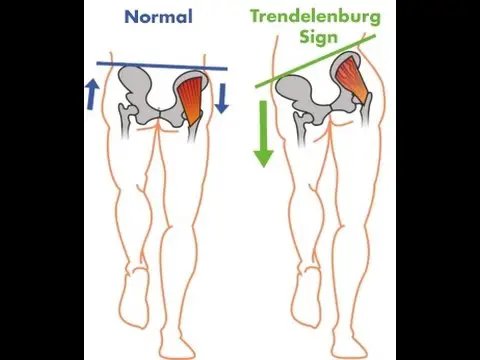
- The Trendelenburg sign is produced when the patient is asked to stand unassisted on each leg in turn. In a positive sign, pelvic drop will occur on the unsupported leg.
- Pelvic drop can be recognized by observing the level of the iliac crests on both sides.
- For example, if the left gluteal muscles are weak, the right side of the pelvis will drop when the patient stands on their left leg (and the right leg is unsupported).
2. Inferior gluteal nerve:
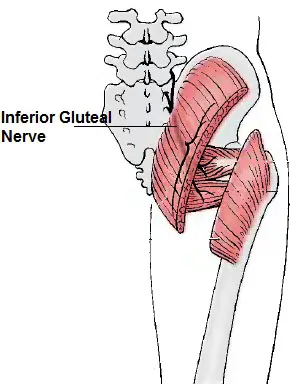
The inferior gluteal nerve is the main motor neuron that innervates the gluteus maximus muscle.
It is responsible for the movement of the gluteus maximus in activities requiring the hip to extend the thigh, such as climbing stairs.
Injury to this nerve is rare but often occurs as a complication of the posterior approach to the hip during hip replacement.
When damaged, one would develop a gluteus maximus lurch, which is a gait abnormality that causes the individual to ‘lurch’ backward to compensate for lack of hip extension.
Anatomy of Inferior gluteal nerve:
The largest muscle of the posterior hip, gluteus maximus, is innervated by the inferior gluteal nerve.
It branches out and then enters the deep surface of the gluteus maximus, the principal extensor of the thigh, and supplies it.
Origin:
The muscle is supplied by the inferior gluteal nerve which arises from the dorsal branches of the ventral rami of the fifth (L5), the first (S1), and second (S2) sacral nerves.
The lumbosacral trunk, which is made up of L5 and a small branch of L4, effectively connects the lumbar and sacral plexuses. The lower branches of the L4 and the L5 nerves enter the sacral plexus.
The sacral plexus is formed by the lumbosacral trunk, the first to third sacral ventral rami, and part of the fourth, the remainder of the last joining the coccygeal plexus.
The sacral plexus is formed in the pelvis in front of the piriformis muscle.
The sacral plexus is formed anterior to the piriformis muscle and gives rise to the sciatic nerve, the superior and inferior gluteal nerves, and the pudendal and posterior femoral cutaneous nerves.
Most of the sacral plexus nerves are scarcely recognizable because they leave the pelvis through the greater sciatic foramen. From the pelvis, the anterior primary branches of the nerves entering the plexus (the first sacral nerve being a particularly large one) and a mass of nerves on the piriformis can be recognized.
Course of Inferior Gluteal Nerve:
- The inferior gluteal nerve leaves the pelvis through the greater sciatic foramen and runs underneath the piriformis muscle.
- It then divides into muscular branches to supply the gluteus maximus that pass posteriorly into the deep surface of the gluteus maximus muscle.
- The inferior gluteal nerve is superficial to the sciatic nerve. It has been described as having multiple branches with subsequent innervation of the overlying gluteus maximus.
- The inferior gluteal nerve entered the deep surface of the gluteus maximus very inferiorly. At the lower border of the piriformis muscle, the nerve turns backward and divides into upward and downward diverging branches, which enter the gluteus maximus.
- The nerve may also send a branch to the posterior femoral cutaneous nerve.
- The inferior gluteal nerve reliably emerged inferior to the piriformis muscle. The branching characteristics of the nerve fall into two broad categories.
- One category is short stalks which came under the piriformis and then gave rise to all of the terminal branches of the nerve which spanned the muscle of the gluteus maximus. The number of branches from the stalk ranged from four to six.
- The second category occurs as a partial split of the stalk that occurred proximal to the coverage of the piriformis.
- There were two to three divisions of the inferior gluteal nerve under the piriformis that would further divide close to the insertion of the nerve into the actual muscle belly.
- The nerve was always seen close to and medial to the sciatic nerve when it left the sacral plexus inferior to the piriformis.
- In all specimens, the nerve entered the deep surface of gluteus maximus approximately 5 cm from the tip of the greater trochanter of the femur and entered the deep surface of gluteus maximus over the inferior one-third of the muscle belly.
- The inferior gluteal nerve is accompanied by the inferior gluteal artery, a branch of the anterior trunk of the internal iliac artery.
- No consistent relationship between the inferior gluteal artery and the inferior gluteal nerve was observed in current studies.
- There is a relationship between the common stalk of the inferior gluteal nerve and external anatomic landmarks.
- The targeted region should be aimed inferior to the most prominent aspect of the greater trochanter, and medial to the landmark of the ischial tuberosity, at the depth of the posterior border of the proximal femur.
- Triangulating using these three coordinates, one can reliably reach the source of the inferior gluteal nerve.
- This will result in maximal stimulation of the gluteus maximus musculature when using electrical stimulation for the purpose of prevention of pressure ulcers.
- The sciatic nerve (L4 to S3), the largest nerve of the body, immediately leaves the pelvis through the greater sciatic foramen, below the piriformis.
- The superior gluteal nerve passes backward through the greater sciatic foramen, above the piriformis.
- The inferior gluteal nerve also passes backward through the greater sciatic foramen but below the piriformis.
Function:
- The major function of the gluteus maximus is to extend the flexed thigh and bring it in line with the trunk.
- It may prevent the forward momentum of the trunk from producing flexion at the supporting hip during bipedal gait.
- It is intermittently active in the walking cycle and in climbing stairs and continuously active in strong lateral rotation and abduction of the thigh and also stabilizes the femur on the tibia when the knee extensors are relaxed.
- In addition to this, the gluteus maximus has an important role during some activities like running or standing up.
- The gluteus maximus, a large muscle with numerous attachments, is a powerful extensor of the thigh or of the trunk lower limbs are in a fixed position.
- The gluteus maximus is also a strong hip stabilzer. It extends the thigh at the hip and assists in laterally rotating the thigh.
- It contracts at heel strike, slowing the forward motion of the trunk by arresting flexion of the hip and initiating extension. This movement prevents the trunk from falling forward.
- Surprisingly, however, the gluteus maximus muscle is not important posturally, is relaxed when one is standing, and is little used in walking.
- It is employed in running, climbing, and rising from a sitting or stooped position. It also controls flexion at the hip upon sitting down.
Clinical Importance:
From hip replacement:
- Inferior gluteal entrapment neuropathy is rarely reported but is recognized as a complication of the posterior approach to hip arthroplasty. Injuries to the peripheral nerves occur in 0.5% to 8% of patients undergoing total hip replacement.
- It is subject to injury by compression and ischemia in sedentary individuals, resulting in difficulty in rising from a sitting position and difficulty climbing stairs.
- The incidence of damage to the inferior gluteal nerve after replacement of the hip is still uncertain.
- Peripheral nerve injury may occur during operations on the hip as a result of operative trauma associated with stretching and retraction of the nerve.
- Few studies have focused on damage to the inferior gluteal nerve during hip replacement.
- In ten other patients who had a posterior approach, nine had abnormal electromyographic findings in inferior gluteal innervated muscles and eight of the ten also had abnormalities in superior gluteal innervated muscles.
- They suggested that abnormalities of gait after the operation may be due to injury to these nerves.
- The reduction in walking speed and persistently abnormal gait, sometimes seen in patients one year after total hip replacement, was associated with a decrease in the extensor moment with a resultant decrease in the range of extension of the hip and a reduction in the abductor moment.
- The posterior approach is the most common and practical of those used to expose the hip joint.
- The posterior approaches allow excellent visualization of the femoral shaft, thus are popular for revision joint replacement surgery in cases in which the femoral component needs to be replaced.
- The likelihood of damage to the inferior gluteal nerve is reported to be high when a muscle-splitting incision is made across the gluteus maximus as a part of the classical posterior approach to the hip.
- This may cause selective denervation of the gluteus maximus since the inferior gluteal nerve courses along the deep surface of the muscle and is not easily visualized and differentiated from other structures running with it, such as blood vessels.
Gluteus maximus lurch:
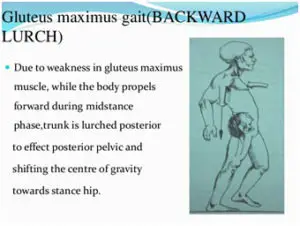
- Injury to this nerve leads to a gluteus maximus lurch. When the gluteus maximus is weak/injured, the trunk extends (lean back) on the heel strike on the weakened side. This compensates for the weakness of hip extension.
- Damage to the inferior gluteal nerve causes loss of extension at the hip and causes the buttock to waste.
- The normal gluteus maximus gait is when the gluteus maxims begin to contract at the moment of heel strike, slowing the forward motion of the trunk by arresting flexion of the hip and initiating extension.
- When the gluteus maximus is weak, the trunk lurches backward (gluteus maximus lurch) at heel-strike on the weakened side to interrupt the forward motion of the trunk.
- There is great difficulty in preventing the flexion of the trunk heel strike so the person may use trunk extension before the heel strike to maintain balance causing a backward lurch. The trunk lurches back on the stance phase side hyperextending.
- The backward trunk lurch persists throughout the stance to maintain the gravitational force line behind the hip axis locking the hip into extension.
- There is an apparent forward protrusion of the affected hip due to exaggerated hip motion and the person may also hold the shoulders backward to keep the center of gravity behind the joint.
- The hamstring muscles often compensate for the gluteus maximus weakness resulting in a near-normal gait pattern but most often these muscles are affected together.
FAQ
What are gluteal nerves?
The dorsal divisions of the L4, L5, and S1 nerve roots of the sacral plexus give rise to the superior gluteal nerve, which is located in the lower pelvis. The tensor fasciae latae, gluteus medius, and gluteus minimus muscles are innervated by the superior gluteal nerve.
Is superior gluteal nerve sensory?
Originating in the pelvis, the superior gluteal nerve is a mixed (motor and sensory) nerve of the sacral plexus. It has a cutaneous branch and innervates the gluteus medius, gluteus minimus, tensor fasciae latae, and piriformis muscles.
What plexus is the gluteal nerve?
the sacral plexus
Divisions of the fifth lumbar through the second sacral nerve are carried by the inferior gluteal nerve, which is a part of the sacral plexus.
What is the pathway of the gluteal nerve?
The posterior divisions of the L4, L5, and S1 anterior roots give rise to the superior gluteal nerve, a motor branch of the sacral plexus. Along the journey, it travels through the superior gluteal artery and vein in addition to the larger sciatic foramen.
What nerve causes hip drop?
When a patient suffers hip abductors paresis or paralysis, they experience Trendelenburg gait. Neuronal injury to the superior gluteal nerve resulting from nerve entrapment or iatrogenic causes might induce hip abductor weakness.