
Muscles Of Forearm
Introduction
The forearm is a vital anatomical region located between the elbow and the wrist. It contains a complex network of muscles that contribute to the intricate movements of the hand, wrist, and fingers. These muscles can be broadly classified into anterior (flexor) muscles and posterior (extensor) muscles.
The anterior muscles facilitate actions such as flexing the wrist and fingers, while the posterior muscles enable wrist and finger extension. These muscles work in synergy to allow activities like grasping, gripping, writing, and various fine motor skills. Understanding the forearm muscles is essential for comprehending the mechanics of upper limb movement and function.
The portion of the upper limb that runs from the elbow to the wrist is known as the forearm. The radius and ulna contribute for creating the forearm’s bony structure. Twenty muscles function on the elbow and wrist joints, as well as the carpometacarpal, metacarpophalangeal, and interphalangeal joints of the hand, in two muscular compartments, the anterior (flexor) and posterior (extensor).
Therefore, the forearm muscles are essential for the upper limb’s fine motor activities, allowing complex motions of the arm, wrist, and fingers.
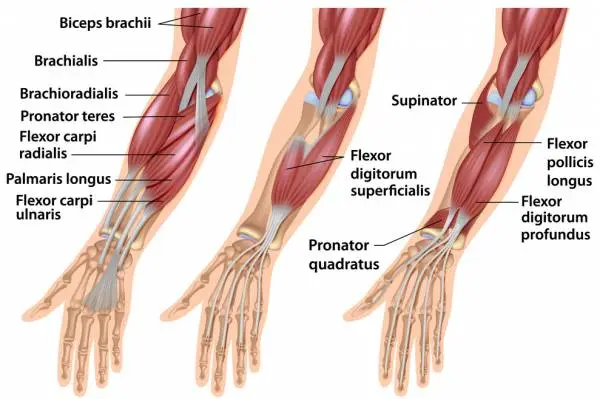
The anterior compartment of the forearm muscle
There are three layers of muscles in the forearm’s anterior compartment: superficial, intermediate, and deep. This muscle group also contributes to wrist flexion, finger flexion, and forearm pronation. They are mostly innervated by the median nerve (excluding the flexor carpi ulnaris muscle and medial half of flexor digitorum profundus muscle, which are supplied by the ulnar nerve), and they acquire arterial supply from the ulnar artery and also the radial artery.
The superficial layer of the anterior compartment
- Flexor carpi ulnaris
- Palmaris longus
- Flexor carpi radialis
- Pronator teres
An intermediate layer of the anterior compartment
Flexor digitorum superficialis
A deep layer of the anterior compartment
- Flexor pollicis longus
- Flexor digitorum profundus
- Pronator quadratus
The superficial layer of the anterior compartment
The superficial layer :
The flexor carpi ulnaris, palmaris longus, flexor carpi radialis, and also pronator teres muscles are the four muscles found in the superficial layer of the anterior compartment of the forearm. The medial epicondyle of the humerus, known as the common flexor tendon, is the origin of all four muscles.
Flexor carpi ulnaris
The flexor carpi ulnaris muscle is the considerable medial muscle in the superficial layer of the forearm. It is a relatively broad and strap-like muscle that recreates a powerful role in movements at the wrist.
- Origin: The flexor carpi ulnaris muscle originates at the medial epicondyle, olecranon process, and posterior border of the ulna.
- Insertion: The flexor carpi ulnaris muscle inserts pisiform bone of the hand.
- Innervation: ulnar nerve
- Arterial supply: ulnar artery
- Function: accessory wrist flexion
Palmaris longus
15% of individuals have absent the palmaris longus muscle. When present, it is situated between the flexor carpi radialis and the flexor carpi ulnaris. The forearm muscle, which is the most superficial, has just a little functional purpose. Therefore, tendon transfers are where it is most frequently used.
- Origin: Palmaris longus muscle originates from the medial epicondyle at the humers.
- Insertion: Palmaris longus muscle inserts into flexor retinaculum and palmar aponeurosis via a long, thin tendon.
- Innervation: median nerve
- Arterial supply: ulnar artery
- Function: accessory wrist flexion
Flexor carpi radialis
The flexor carpi radialis is located directly lateral to the palmaris longus when it is present. The radial artery is palpable lateral to the tendon of the flexor carpi radialis as we move more laterally in the forearm.
- Origin: The flexor carpi radialis muscle originates at the medial epicondyle at the humers.
- Insertion: The flexor carpi radialis muscle insertion at the base of the metacarpals II and III.
- Innervation: median nerve
- Arterial supply: radial artery
- Function: wrist flexion and abduction
Pronator teres
The pronator teres muscle forms the medial boundary of the cubital fossa in the anterior elbow. There are two heads on this muscle, which is a functionally significant muscle. Between the two heads of the pronator teres, the median nerve enters the forearm and is separated from the ulnar artery by the ulnar head of the pronator teres.
- Origin: Pronator teres muscle originates from two head-
- Humeral head: originate the medial supracondylar ridge of the humerus
- Ulnar head: ulnar coronoid process
- Insertion: Pronator teres muscle inserts the lateral surface of the distal radius.
- Innervation: median nerve
- Arterial supply: brachial artery
- Function: pronation of the forearm
An intermediate layer of the anterior compartment
Flexor digitorum superficialis is just one muscle found in the intermediate layer. Although it is occasionally categorized as a superficial muscle, in most people it is located in the middle of the deep and superficial muscle layers. The muscle is a useful anatomical landmark in the forearm because the ulnar artery and median nerve pass between its two heads before proceeding posteriorly.
Flexor digitorum superficialis
The flexor digitorum superficialis muscle has several essential characteristics. Proximally, The two heads of the flexor digitorum superficialis, the radial and humero-ulnar, are located on either side of the median nerve and ulnar artery. Four tendons from the flexor digitorum superficialis separate distally and travel via the carpal tunnel to the digits II, III, IV, and V. The tendon divides into two at the proximal phalangeal base of fingers II through V, passing laterally and then posteriorly across the tendon of the flexor digitorum profundus before joining the lateral borders of the middle phalanx.
- Origin: The flexor digitorum superficialis muscle originates from two head –
- Humeroulnar head: medial epicondyle
- Radial head: anterior oblique line of the radius bone.
- Humeroulnar head: medial epicondyle
- Insertion: The flexor digitorum superficialis muscle inserts the middle phalanx of digits II-V
- Innervation: median nerve
- Arterial supply: Medial aspect: ulnar artery
- Lateral aspect: radial and median arteries
- Function: flexion at the proximal interphalangeal joint, metacarpophalangeal, and wrist joints
A deep layer of the anterior compartment
The deep layer includes three muscles at deep layer: Flexor pollicis longus, Flexor digitorum profundus, Pronator quadratus
Flexor pollicis longus
Strong thumb flexor, the flexor pollicis longus muscle transmits a long, single tendon across the lateral part of the carpal tunnel.
- Origin: The flexor pollicis longus muscle originates the anterior surface of the radius bone and interosseous membrane.
- Insertion: The flexor pollicis longus muscle insertion at the base of the distal phalanx of the thumb area.
- Innervation: supplied by the anterior interosseous nerve from the median nerve
- Arterial supply:
- Proximal aspect: anterior interosseous artery
- Distal aspect: radial artery
- Function: flexion of the thumb
The flexor digitorum profundus is a powerful finger and wrist flexor that is one of numerous essential elements in both grip strength and executing a pincer grasp. It has four tendons that pass through the inferior region of the carpal tunnel before separating to digits II-V, where it passes via the tunnel created by the splitting of the tendons of flexor digitorum superficialis.
- Origin: The flexor digitorum profundus muscle originates anterior and medial surface of the ulna and adjacent interosseous membrane
- Insertion: The flexor digitorum profundus inserts the anterior surface of the base of the distal phalanx of digits II-V
- Innervation:
- Medial aspect: ulnar nerve
- Lateral aspect: supplied by the anterior interosseous nerve from the median nerve
- Arterial supply: ulnar and anterior interosseous arteries
- Function: flexion of the distal and proximal interphalangeal, metacarpophalangeal, and also wrist joints motion
Pronator quadratus
The pronator quadratus is a flat square-shaped muscle in the distal forearm that assists and stabilizes the forearm pronation produced by pronator teres.
- Origin: It arises at the anteromedial surface of the distal ulnar area.
- Insertion: The pronator quadratus muscle inserts the anterolateral surface of the radius
- Innervation: supplied by the anterior interosseous nerve from the median nerve
- Arterial supply: anterior interosseous artery
- Function: pronation and stabilization of the forearm
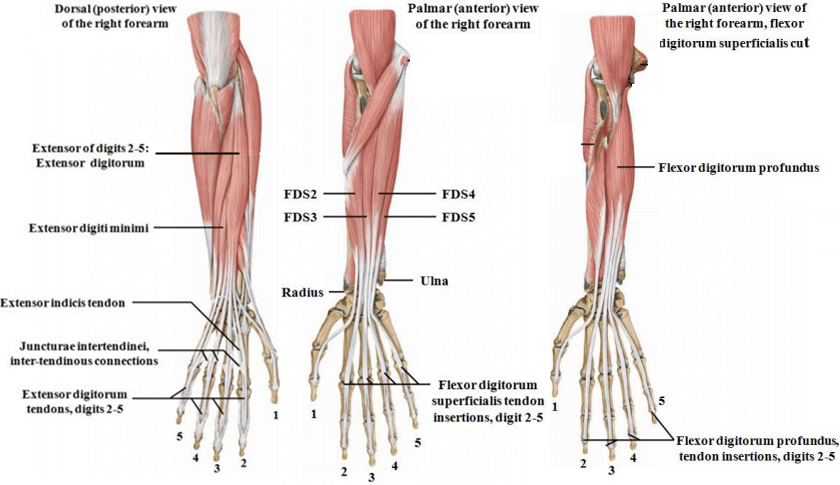
The posterior compartment of the forearm muscles
Extensor muscles are the general name for the muscles in the back of the forearm. These muscles’ primary purpose is to provide wrist and finger extension. The radial nerve innervates each one of them. Wrist and/or finger extension, as well as thumb abduction, are produced by the muscles in the posterior compartment of the forearm. There are two layers of muscles in this compartment: deep and superficial. A fascia layer lies between these two layers.
The superficial layer of the posterior compartment
- Brachioradialis
- Extensor carpi radialis longus
- Extensor carpi radialis brevis
- Extensor digitorum
- Extensor digiti minimi
- Extensor carpi ulnaris
A deep layer of the posterior compartment
- Supinator
- Abductor pollicus longus
- Extensor pollicus longus
- Extensor pollicus brevis
- Extensor indicis
The superficial layer of the posterior compartment
There are seven muscles in the superficial layer of the posterior compartment of the forearm that all originate from the supracondylar ridge and the lateral epicondyle of the humerus (the common extensor tendon): Extensor digitorum, Extensor digit minimi, Extensor digitorum longus, Extensor digitorum brevis, Brachioradialis, and Extensor carpi ulnaris muscles.
Brachioradialis
The Brachioradialis muscle creates only moderate elbow flexion but becomes active as a powerful elbow fixator (as while holding a box in front of you). It is the only muscle in the posterior forearm compartment that causes flexion at a joint, and it is most effective when somewhat pronated. The radial nerve divides here before entering this muscle deeply, and the brachioradialis forms the lateral border of the cubital fossa.
- Origin: The Brachioradialis muscle originates the proximal third of the lateral supracondylar ridge at humers.
- Insertion: The Brachioradialis muscle inserts at or immediately proximal to the radial styloid process.
- Innervation: radial nerve
- Arterial supply: radial recurrent
- Function: weak elbow flexion; primary elbow fixator
Extensor carpi radialis longus
The extensor carpi radialis longus has a longer tendon and a relatively long muscle belly. The extensor carpi radialis brevis is distinguishable from it by the length of its tendon and its outward appearance.
- Origin: The Extensor carpi radialis longus muscle lateral supracondylar ridge and lateral epicondyle at humers.
- Insertion: The Extensor carpi radialis longus muscle inserts the dorsal surface of the metacarpal II bone.
- Innervation: supplied by the radial nerve before bifurcating into superficial and deep branches
- Arterial supply: radial recurrent artery
- Function: wrist extension and abduction
Extensor carpi radialis brevis
The extensor carpi radialis brevis, the smaller sibling of the extensor carpi radialis longus, is distinguished by its deeper appearance to the extensor carpi radialis longus and its shorter tendon that appears to have a larger muscle belly. Before the radial nerve passes through the supinator, it is the last superficial muscle of the posterior forearm that it supplies.
- Origin: The Extensor carpi radialis brevis muscle lateral epicondyle of the humerus.
- Insertion: The Extensor carpi radialis brevis muscle insertion at the base of metacarpals II and III.
- Innervation: radial nerve
- Arterial supply: radial artery
- Function: extension and abduction of the wrist
Extensor digitorum (communis)
The extensor digitorum muscle has the major extensor muscle of digits II-V. This muscle originates from a very short common muscle belly that divides into four separate muscle bellies, each of which produces a single tendon. On the dorsal surface of each digit, each tendon inserts into the connected triangle aponeurosis (dorsal hood, extensor expansion).
- Origin: The extensor digitorum muscle arises from the lateral epicondyle of the humerus bone.
- Insertion: The extensor digitorum muscle inserts at the extensor expansion of the dorsal hand.
- Innervation: posterior interosseous nerve
- Arterial supply: posterior interosseous artery
- Function: extension of digits II-V
Extensor digit minimi (extensor digiti quinti proprius)
The little finger’s additional extensor muscle is called the extensor digiti minimi.
- Origin: The Extensor digit minimi originates lateral epicondyle
- Insertion: The Extensor digit minimi inserted extensor expansion, immediately medial to extensor digitorum
- Innervation: posterior interosseous nerve
- Arterial supply: posterior interosseous artery
- Function: extension of digit V
Extensor carpi ulnaris
An essential wrist extensor and adductor is the extensor carpi ulnaris. It has a long, flat tendon that converges distally into a round tendon with a relatively small muscle belly.
- Origin: Extensor carpi ulnarisoriginats at the lateral epicondyle of the humerus.
- Insertion: Extensor carpi ulnaris inserts at the medial aspect of the base of metacarpal V.
- Innervation: posterior interosseous nerve
- Arterial supply: posterior interosseous artery
- Function: extension and adduction of the wrist
Anconeus
The anconeus is a small muscle that supports other muscles in the posterior forearm and is so named because of its triangular shape.
- Origin: The anconeus muscle originates the lateral epicondyle of the humerus.
- Insertion:The anconeus muscle insertes the dorsolateral surface of the olecranon process and dorsal ulna.
- Innervation: radial nerve
- Arterial supply: recurrent interosseous artery
- Function: extension; in pronation, abducts ulna
The deep layer of the posterior compartment
The deep layer of the posterior compartment contains five muscles, all of which are innervated by the posterior interosseous nerve: Supinator, Abductor policies longus, Extensor policies longus, Extensor policies brevis, Extensor indicis, Deep posterior forearm muscles.
The superficial and deep heads of the supinator muscle work together to supinate the forearm. The deep branch of the radial nerve passes between these two heads. This tunnel is known as the Arcade of Frohse because the superficial head serves as its “roof.”
- Origin: The supinator muscle originates from two head
- Superficial head: lateral epicondyle
- Deep head: supinator crest (dorsolateral ulna)
- Insertion: The supinator muscle inserts proximal lateral radius, at or superior to the oblique line.
- Innervation: deep branch of the radial nerve
- Arterial supply: radial recurrent artery
- Function: supination of the forearm
Abductor pollicis longus
The abductor pollicis longus muscle helps in both wrist abduction as well as thumb abduction between metacarpal I and the (os) trapezium. The abductor pollicis longus muscle supports the extensor pollicis brevis in establishing the inferior margin of the anatomical snuffbox.
- Origin: The abductor pollicis longus muscle originates proximal dorsal radius, ulna, and interosseous membrane
- Insertion: The abductor pollicis longus muscle inserts the lateral aspect of metacarpal I.
- Innervation: posterior interosseous nerve
- Arterial supply: Proximal aspect: posterior interosseous artery
- Distal aspect: anterior interosseous artery
- Function: abduction motion of the thumb and assists in abduction at the wrist
Extensor pollicis brevis
Extensor pollicis brevis is the little sibling of extensor pollicis longus. The extensor pollicis brevis takes a shortcut to reach the thumb; the extensor pollicis longus takes the long way to the thumb, passing through the extensor retinaculum. The inferior edge of the anatomical snuffbox is formed by the extensor pollicis brevis working with the abductor pollicis longus.
- Origin: The Extensor pollicis brevis muscle originates the dorsal radius, ulna, and interosseous membrane
- Insertion: The Extensor pollicis brevis muscle insertes dorsal surface of the proximal phalanx of digit I
- Innervation: posterior interosseous nerve
- Arterial supply: posterior interosseous artery
- Function: extension motion of the carpometacarpal joint and metacarpophalangeal joints of digit I assist abduction of the wrist
Extensor pollicis longus
The extensor pollicis longus muscle takes more time to reach the thumb than its little sibling extensor pollicis brevis muscle. Before crossing to the thumb, the extensor pollicis longus circles the dorsal radial tubercle (Lister’s tubercle). The superior border of the anatomical snuff box is formed by the extensor pollicis longus.
- Origin: The extensor pollicis longus muscle arises dorsal ulna and interosseous membrane
- Insertion: The extensor pollicis longus insrets dorsal surface of the distal phalanx of digit I.
- Innervation: posterior interosseous nerve
- Arterial supply: posterior interosseous artery
- Function: extension motion of the carpometacarpal joint and metacarpophalangeal joints of digit I assist abduction of the wrist.
The accessory extensor of the index finger, known as the extensor indices, allows for the index finger’s more fine, more dexterous movement.
- Origin: The extensor indices originate dorsal ulna surfaces.
- Insertion: The extensor indices insert the extensor expansion of digit II (adjacent to the digit II tendon of the extensor digitorum).
- Innervation: posterior interosseous nerve
- Arterial supply: Proximal aspect: posterior interosseous artery
- Distal aspect: anterior interosseous artery
- Function: Mostly an expansion of the second digit at the metacarpophalangeal joint.
Clinical relevance:
Epicondylitis
Extraarticular medial or lateral elbow pain can frequently get worse by repetitive motions. Medial epicondylitis, a condition marked by inflammation and thickened connective tissue in the common flexor tendon at the medial epicondyle of the humerus, is frequently brought on by repeated false strain of the superficial anterior forearm muscles. Due to the constant wrist flexion required for the golf swing, golfers in particular are plagued by the condition. Because of this, this condition is sometimes known as a golfer’s elbow.
Classical symptoms include pain that worsens with movement and difficulty with daily activities (such as shaking hands or pressing a door handle). Notably, medial epicondylitis (also known as “little league elbow”) is a common condition among young baseball players. Children’s bones have ossification centers because they are still growing, which is the cause. When these are subjected to intense false strain, the pressure is transmitted to the apophysis, where it might result in apophysitis or even deformation.
Medial epicondylitis
Localized tenderness over the medial epicondyle and proximal wrist flexors; Pain with resisted wrist flexion with the elbow extended; Pain with passive wrist extension with the elbow extended
Localized tenderness over lateral epicondyle and proximal wrist extensors; Pain with resisted wrist extension with the elbow in full extension; Pain with passive wrist flexion with the elbow in full extension
Intersection syndrome
On the dorsolateral forearm, where the abductor pollicis longus and extensor pollicis brevis muscle bellies cross over the extensor carpi radialis longus and brevis, intersection syndrome is a painful inflammatory condition that develops. This inflammatory condition typically develops as a result of repetitive motions like rowing or weight lifting. The best way to treat intersection syndrome is to avoid aggravating activities and rest, while applying ice or cool compresses can also help reduce inflammation. It is frequently mistaken for De Quervain’s syndrome.
De Quervain’s syndrome
Extensor pollicis brevis and abductor pollicis longus muscles are affected by the inflammatory disorder known as De Quervain’s syndrome. Only these two muscles are affected by this disorder. It is referred to as one of the repetitive strain injuries and is typically brought on by overuse. The dorsal interossei and thumb are both affected by pain that passes down the lateral side of the distal forearm.
It is usually diagnosed clinically with Finkelstein’s test, but MRI can confirm the presence of inflammation and local edema around the tendons of the extensor pollicis brevis and abductor pollicis longus. De Quervain’s syndrome treatment may require some time, and it works best when aggravating injuries are avoided, NSAIDs are used, and cool compresses are applied. Steroid injections are controversial, but plastic surgery can provide a permanent cure.
Treatment
Strengthening exercise:
This strengthening exercise helps you strengthen the muscle of the forearm and decrease the weakness of the forearm.
Palms-up wrist curl:
The patient is seated with their palms facing up and their wrists resting on a flat surface and their knees. A dumbbell is being held by the patient in each hand. After that, raise the hands as high as you can while maintaining the arms steady. The wrist joint should not rise off the surface to indicate that it is in a resting posture. Then, after a brief pause, descend the hands to their starting position.
Palms-down wrist curl:
The patient is seated with their palms facing up and their wrists resting on a flat surface and their knees. The patient must keep a dumbbell in each hand, lift the hands as high as they can, and keep their arms steady. However, if their wrist joint does not rise off the floor, it is in a resting posture. Put the hands back in the starting position after some time.
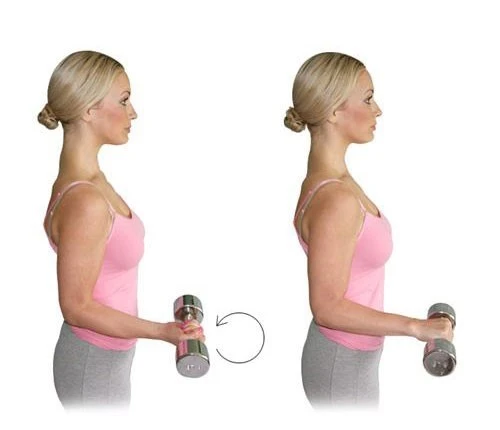
Grip crush:
The patient is sitting with the left wrist joint supported by the knee and a flat surface while holding a dumbbell. The hand should then be relaxed and open so that the dumbbell rolls toward the fingertips. Squeeze the weight as tightly as you can while tensely bending your wrist. After completing the ten repetitions, repeat on the other side
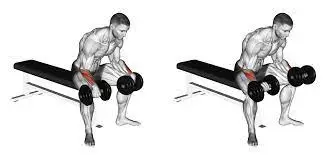
Wrist dumbbell curls:
The patient is positioned holding a slightly heavy dumbbell in each hand while sitting on a bench and chair. Then place the forearms on the thighs with the palms facing upward and the wrists resting on top of the knees. After that, the patient should gradually reduce the weight as far as they can go. Hold the weights firmly and solely make hand motions. The patient should curl the weights as high as they can go before returning to the starting position. Perform this exercise with three sets of 12 repetitions till the muscles complete the exercise. Alternately, complete each side separately.
The pinch-grip plate holds :
The patient’s position is straightforward fingers, pinch and hold a fairly heavyweight plate between the thumb and four fingers of the hand. But one side of this exercise is completed at a time. As long as the patient can, hold this position for 30 to 45 seconds every set. After completing the exercise, take a moment to rest before doing it again.
Reverse barbell curl with the thumb-less grip:
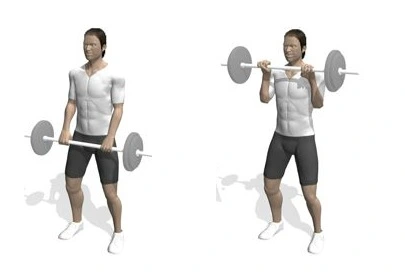
The patient is standing and holding a barbell with his or her hands shoulder-distance apart and palms facing down. The “thumbless grip” is maintained by keeping the thumb with the other fingers. The barbell is then slowly lowered toward the shoulders with the elbows kept close to the sides. Then, to concentrate on the forearms, perform only flexing at the elbow joint. Return to the beginning position and proceed the full time by moving too slowly to perform the three sets of 12 repetitions each day after that.
Elbow bend:
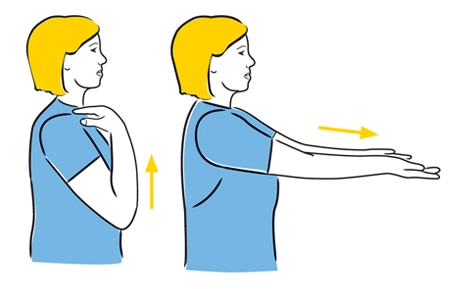
The patient is standing position when performing the wrist extension exercise. The affected arm is then extended forward until it is parallel to the ground. Pull the wrist joint back toward the body with the help of the other hand, then pull it back until there is a stretch in the forearm muscle but no pain. Ten times daily, hold this position for 15 to 30 seconds while performing the activity.
Wrist extension:
The patient is standing when performing the wrist extension exercise. The affected arm is then extended forward until it is parallel to the ground. Pull the wrist joint back toward the body with the aid of the other hand, then pull it back until you feel a stretch in the forearm muscle but no pain. Ten times daily, hold this position for 15 to 30 seconds while performing the exercise.
elbow extension
The patient’s position is that of a seated position for the Elbow extension exercise. With the other hand, gently push the forearm down toward the table or ground while placing the elbow on a chair or table arm. Hold this position for 15 seconds while experiencing a stretch but no pain. Ten times a day, repeat this exercise.
Wrist rotations:

For the wrist rotations, the patient is positioned in a sitting position. The patient made a fist and rotated each wrist counterclockwise and then clockwise in a circular motion while holding their arms out in front of them at shoulder height. Perform this exercise 10 times daily, once in each direction.
Forearm squeeze:

In such a position, the patient will hold a tennis ball or sock between their forearms while also using another object to squeeze. To squeeze the object, extend and flex your fingers. Hold the position for 3 to 5 seconds, then release the grip of the grasp for a little while. Do this exercise two to three times daily, for a total of 10 to 15 minutes at a time.
Fingertip push-ups:
The patient’s position is kneeling by a bench and a strong object and bringing the fingertips down on the surface. The patient next lowers their chest to the bench while maintaining control, bending their elbow at a 90-degree angle. Do this exercise in two to three sets of eight to twelve repetitions before returning to the beginning position.
Crab walk:
A reverse tabletop position is taken by the patient. Align the ankle joint directly under the knee joint and place the hands under the shoulder joint with the fingers pointing in the direction of your feet. After then, move forward for up to a minute at a time while using only your hands and feet. three to four times per day, do this exercise.
Plank with shoulder taps:

The patient is lying on a yoga mat while kneeling on the ground. As in a pushup, place the hands squarely under the shoulder joint. Next, curl your toes under and raise your body into a plank position. Must maintain core stability, lift the right hand off the floor, and touch the opposite shoulder. Then gradually return to your starting position. As long as the patient is able, perform this exercise for 30 to 60 seconds and then repeat it 2 to 3 times daily.
Isometric wall push :
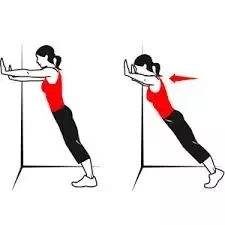
The patient is in a standing position in front of the wall with their hands on the wall. They are maintaining arm straightness without locking the elbow joint. Then, for 15 to 30 seconds, press them hard against the wall. After 30 seconds, remove the pressure. Accomplish this exercise two to three times per daytime.
Sphinx push-ups :
The patient begins in a forearm plank position, either on their toes or their knees. Following that, forcefully press the hands down while attempting to raise the forearms till they are straight. Then use the control to descend once again. Just move an inch or two at a time if you can’t move at once. Release the pressure, then perform this exercise two or three more times daily.
Pull-up bar hang:
The patient should begin by placing their hands on the pull-up bar, shoulder-width apart, with their palms facing forward. Hold the position with your arms straight and your ankles crossed behind you for up to 15 to 30 seconds. Repeat this exercise 2 to 3 times daily after the release. Then, to make it more difficult for this exercise, wrap two tiny towels around the bar and grip on to that.
Stretching exercise :
Wrist Extension Stretch:
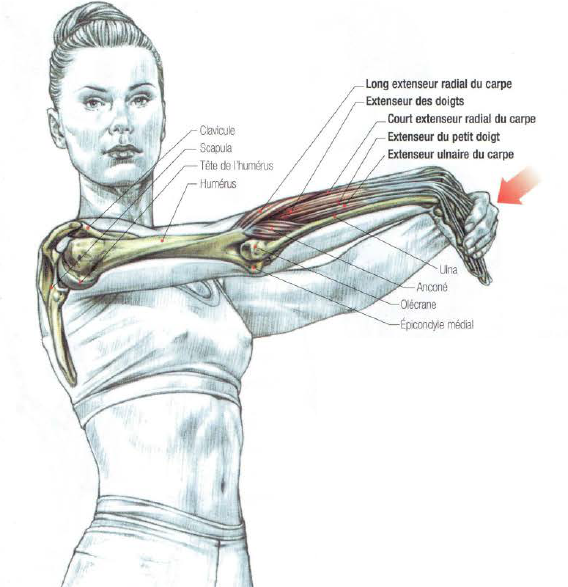
For the stretching, the patient is in a sitting or standing position. After holding the arm out parallel to the floor, the patient extends from the shoulder. The hand is now looking downward following the turn. Utilize the hand that pulls the hand that is extended down and toward the body. Flexing the wrist joint will cause the top of the hand and forearm to feel stretched; next, turn the arm slightly inward to feel a second stretch. Hold this stretching exercise position for 15 to 20 seconds. Five times on each side, repeat this stretching exercise.
Forearm flexor stretch:
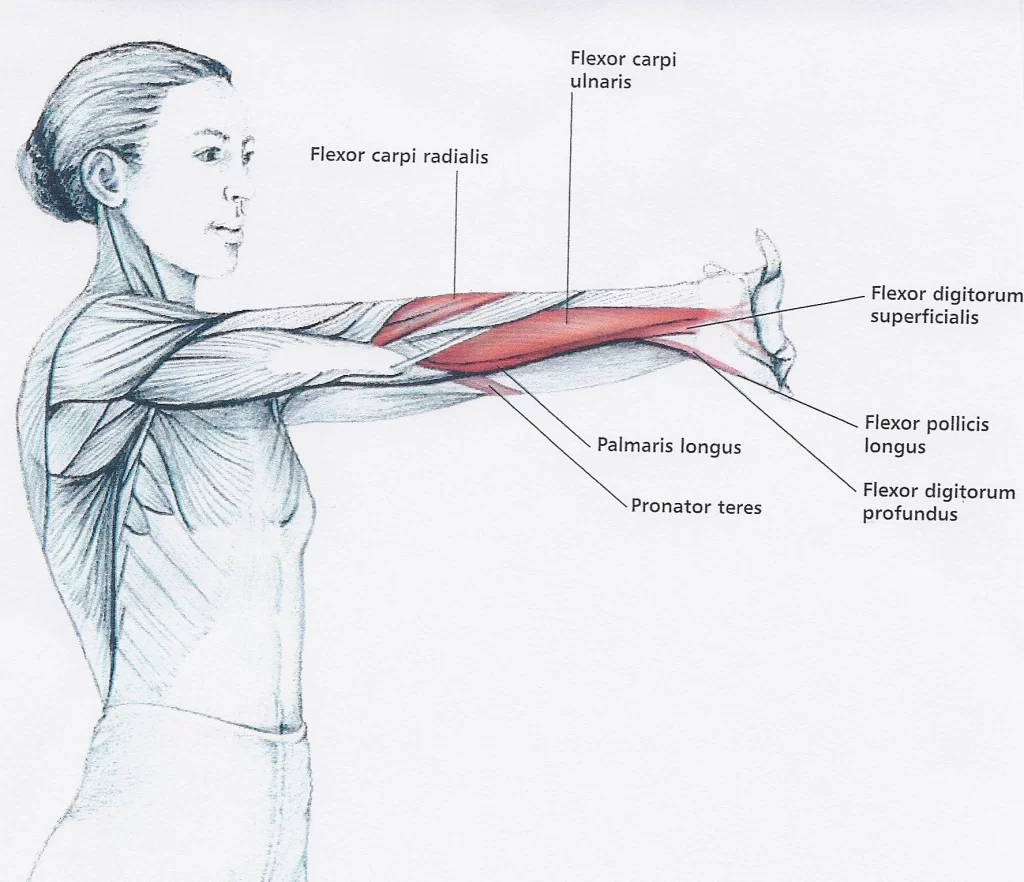
For this stretching, the patient is in a standing position. Put one hand up in the air like you’re waving to a friend while holding both arms out in front of the body with the elbow joints locked out. The fingers should then be gently pulled toward the body with the opposing hand. Maintaining this stretching exercise should take 15 to 20 seconds. The other arm should then receive the same stretching exercise.
Supinator stretch:
The patient position is in a sitting position for supinator stretching exercise. Keep a light dumbbell in one hand and place the other end on a flat surface with the palm down. the hand should then be allowed to rotate the dumbbell slightly beyond neutral. Maintaining this stretching exercise should take 15 to 20 seconds. Five times on each side, repeat this stretching exercise.
Two-arm forearm stretch:
The patient should stand position with their hands extended in front of them, elbows locked out, and internally rotate—that is, rotate their shoulders in a medial direction—so that their palms are facing each other on the backs of their hands. the fingers of both hands should be interlocked before placing one hand over the other. As the arm is extended, rotate the arms in the other direction, and then, using the arm that isn’t being used, flex the wrist joint of the extended arm. Repeat this stretching exercise on the opposite arm by moving to the top position after maintaining it for 15–20 seconds.
Praying forearm stretch:
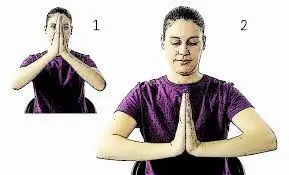
The patient is in a standing position and is sitting upright in a chair. Put both hands together with the palms facing each other but without locking the fingers, and then elevate both elbows so that the wrist joint starts to flex. After that, continue to raise the elbow joint until you feel a wonderful stretch in the underside of the forearms. Maintaining this stretching exercise should take 15 to 20 seconds. Five times on each side, repeat this stretching exercise.
FAQs
What are the muscles in the forearm of the hand?
The muscles that originate from the front forearm and insert into the hand can be further divided into three categories: superficial, intermediate, and deep groups. Flexor muscles make up the majority of the group of muscles. The flexor carpi radialis, palmaris longus, and flexor carpi ulnaris are include of the superficial group.
What is the largest muscle in the forearm?
The largest and most superficial muscle in the forearm is the brachioradialis. Working them will therefore have the biggest impact on how your forearm appears.
What is the rare muscle in the forearm?
Although it is not always present, the palmaris longus is a muscle that can be seen as a small tendon that lies between the flexor carpi radialis and the flexor carpi ulnaris. About 14% of people lack it; however, this percentage varies among African, Asian, and Native American populations.
What are the three exercises for forearms?
The reverse curl, wrist curl, and wrist extension are the three most effective exercises for that. These three movements combined constitute the basis of a full forearm exercise. The huge barbell exercises can easily beat up our hands because grip and forearm strength are frequently already limiting problems for beginner lifters.
How do you treat a forearm injury?
RICE treatment Therapy involving rest, ice, compression, and elevation can help reduce pain and inflammation in the forearm’s damaged tendons and muscles. Pain medications: Forearm pain symptoms may be relieved by over-the-counter medicines.
Why do forearm exercises?
Exercises for the forearms concentrate on strengthening the muscles that cross over your wrists, hands, and elbows, which helps you be more productive throughout the day. A stronger grip makes it easier for you to use your hands and arms to lift, hold, move, and transfer objects.


2 Comments