PARAPLEGIA
What is Paraplegia?
- It is define as paralysis or loss of motor function in both lower extremities with or without sensory impairment .
- It is usually caused by involvement of cerebral cortex , spinal cord and nerves supplying the muscles of lower extremities.
- If there is complete paralysis of both lower limb – called PARAPLEGIA
- If there is only weakness present then – called PARAPARESIS.
Causes of Paraplegia :
- Paraplegia may occurs due to UMN or LMN lesion,gunshot injury,car accident,falls,sports accidents etc.
- Upper motor neuron lesion:-
1) Intracranial causes :
Tumors of falx cerebri
Thrombosis of superior sagittal sinus
- Thrombosis of unpaired anterior cerebral artery affecting both leg area
2)Spinal causes :
Trauma
Multiple sclerosis
Epidural abscess
Radiation myelopathy
Acute transverse myelitis
Hereditary spastic paraparesis
Motor neuron disease like amyotrophic lateral sclerosis
Fracture dislocation of the thoracic or lumbar vertebrae
Compression of the cord by space occupying lesion
Pott’s paraplegia following tuberculosis of the spine
Subacute combined degeneration of the cord
Vascular causes like hemorrhage,thrombosis,arteriovenous malformation - Lower motor neuron lesion:-
Myasthenia gravis
Spina bifida with myelomeningocele
Roots lesion like in cauda equina syndrome
Muscular condition like muscular dystrophies,polymyositis
Peripheral nerve lesion such as in neuropathies,polyneuritis
Anterior horn cell lesion like poliomyelitis,spinal muscular atrophy and motor neuron disease.
Types of Paraplegia :
- It depend on intact connections between the reticular formation nuclei and the spinal cord and involvement vestibulospinal and rubrospinal tract.
- 1)Paraplegia in extension :
- If the spinal lesion in partial so as to spare the reticulospinal tract, extensor hypertonia predominates.Occasionally flexor withdrawal reflex is elicited on giving noxious stimulus.there are pyramidal tracts involved only and early recovery occured.
- 2)Paraplegia in flexion :-
- If the spinal lesion destroys not only corticospinal tract but also reticulospinal tract, flexor withdrawal reflex is freed from its antagonists and shows domination. Lower limb takes flexion attitude. Both pyramidal and extrapyramidal tracts are involved. Recovery period is longer than paraplegia in extension.
What is the Spinal cord Injury?
- Damage to the spinal cord that results in a loss of function such as mobility or feeling of sense.
- It causes temporary or permanent changes in its function.
- Symptoms may include loss of muscle function, sensation, or autonomic function in the parts of the body served by the spinal cord below the level of injury.
Types of spinal cord injury according to injury:
- 1)Incomplete or partial injury: Spinal cord is able to convey some messages to or from the brain.
- Therefore,retain some sensation and possibly some motor function below the affected area.
- Complete recovery is possible.
- 2)Complete injury : There is complete loss of motor function and sensation below the area of injury.
- Complete recovery may or may not be possible.
Causes of spinal cord injury:
- Road traffic accidents
- Bullet or stab wound injury
- Traumatic injury like vertebral fracture,compression or wedge fracture
- Electric shock
- Extreme twisting of the middle of the body
- Landing on the head during a sports injury
- Fall from a great height
Incidence: It is highest among persons age between 16-30 years and males are more prone to SCI.
Pathophysiology of Paraplegia and Spinal cord Injury :
- Soon after spinal cord injury,some vascular and biochemical changes occurs which leads to infarction which in turn leads to necrosis.
- Infarction could be due to either direct injury to the spinal cord arteries or due to certain biochemical events that leads to hypoxia which causes edema and infarction.
- any trauma to the spinal cord leads to release in non-epinephrine which is a vasoconstrictor causing infarction
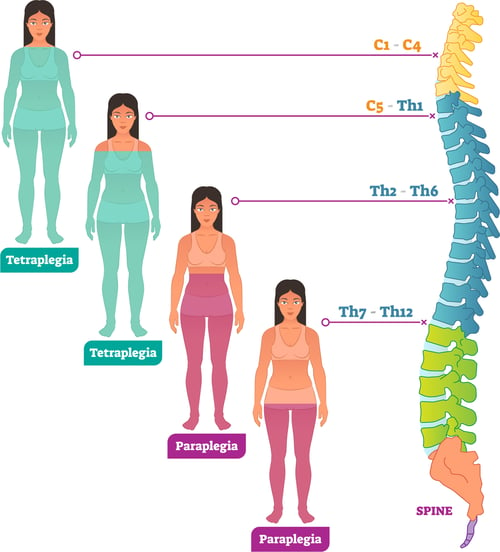
What are the level of spinal cord injury causes Quadriplegia & Paraplegia ?
- Occurrence of quadriplegia and paraplegia may depend on which level of spinal cord injury present.
- Quadriplegia is define as complete paralysis of both upper limbs and lower limbs.It occurs when there is injury present at cervical level. paraplegia occurs when injury present at thoracic and lumbar level.
- QUADRIPLEGIA :
- C1-4 quadriplegia
- C1 and C2 may have functional phrenic nerves.
- C3 – There is breathing difficulty and ventilator dependent patient.
- C4 – May be free from advance respiratory support but require functional equipment need as C3.
- C1-4 quadriplegics require assistance for all personal care,bed mobility,and transfer function.
- C5 quadriplegia
- -Have functional deltoid and biceps muscle.
- Can feed themselves, perform oral facial hygienic and upper body dressing activities.
- Require assistance to perform bathing,bowel and bladder care and for transfer.
- C6 quadriplegia
- Have most of the shoulder muscle normal.
- Elbow bending is normal but not straightening and active wrist extension.
- Can perform upper and lower body dressing without assistance.
- Can perform some transfer independently with a transfer board.
- C7-8 quadriplegia
- Have functional elbow muscle.
- May also have enhanced finger extension and wrist flexion.
- They can turn and perform most transfers independently.
- PARAPLEGIA :
- T1-8 level
- -Retain control of the arms and hands.
- -Poor trunk control and balance due to poor abdominal muscle control.
- T9-12 level
- -Good trunk control and good abdominal muscle control.
- Sitting balance of people with lower spinal cord injuries is usually good.
- Lumbar and sacral injuries result in decreased control of the hip flexor and legs.
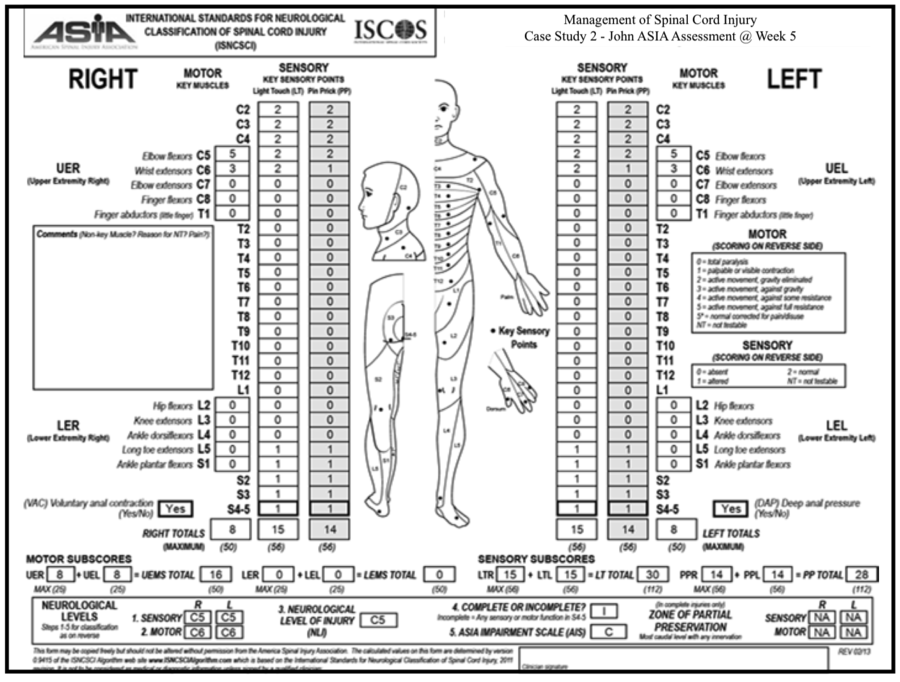
- Level of spinal cord injury also decided using ASIA scale.

Signs and Symptoms :
- Immediately after injury, there is a stage of spinal shock:
- Spinal shock is a state of areflexia characterised by loss of tone, loss of reflexes and total inactivity.
- This is last for 24 hours to week but usually resolved within 24 to 48 hours.
- The first indicator of the resolving spinal shock is the presence of bulbocavernous reflex elicited both in males and females.
- After spinal shock has passed the various neurological signs and symptoms present which are of the following :
- loss of sensory and motor function
- loss of thermoregulatory functions
- Spasticity
- Bowel and bladder dysfunction- Autonomous or areflexic bladder
- sexual dysfunction like loss of libido,difficulty in ejaculation and eraction
- Respiratory dysfunction -Most common cause of death due to spinal cord injury
Complication :
- Pressure sore
- Tightness, contracture and deformity
- Orthostatic hypotension
- Osteoporosis
- Urinary complication like urinary tract infection, renal or bladder calculi
- depression
- Heterotropic bone formation
- Pain syndrome
- Autonomous dysreflexia
- gastrointestinal complication like constipation
What is Hereditary spastic Paraplegia?
- It is a general term used for group of rare inherited disorders that cause weakness and stiffness in the leg muscles.
- Symptoms gradually get worse over time.
- It’s also known as familial spastic paraparesis or strumpell-lorrain syndrome.
- Symptoms :
- The severity and progression of symptoms will vary from person to person.
- A gradual weakness in the legs
- Increased muscle tone and spasticity
- Problems peeing – Such as an urgent need to pee, even when the bladder is not full
- Sometime lack of sensation in the feet.
Difference between Paraplegia and Quadriplegia :
| No. | PARAPLEGIA | QUADRIPLEGIA |
| 1 | Complete paralysis of bilateral lower limb. | Complete paralysis of all four limbs and torso. |
| 2 | Occurs due to thoracic, lumbar and sacral level injury. | Occurs due to cervical level injury. |
| 3 | Upper limb reflexes are normal. | Upper limb reflexes are affected like, hyporeflexia, areflexia, or hyperreflexia. |
| 4 | Breathing problem may or may not present. | Breathing problem is more common. |
| 5 | Function of hands and arms are normal. | Paralysis of hands and partially arms are present. |
| 6 | Speech and swallowing problem are not present. | Speech and swallowing problem are present. |
| 7 | Patient can lives independently with assistance of leg brace and wheelchair. | Patient requires full time care to assist them in day to day activity. |
| 8 | Better prognosis than quadriplegia. | Poor prognosis is present. |
Physiotherapy Treatment :
Aims of physiotherapy Treatment :
- Prevention of all secondary complication as a result of being bedridden.
- Restoration of functional independency to the maximum possible level.
- Psychological counseling.
- Social and vocational rehabilitation.
- Family education and home adaptation.
Counseling :
- A patient who is depressed cannot cooperate with the therapist which will have a negative effect on the overall rehabilitation.
- So that therapist should give appropriate psychological counseling to enable the patient to come out of the state of depression.
- Therapist should try to gain maximum cooperation and highlight the positive features contained in the patient even at this stage which in turn will inspire the patient to look at his future in a more convincing manner.
- Keep in mind that one should not give false hopes to the patient.
- Articles of paraplegic patient leading a independent and even successful life will help in motivating the patient for recovery.
Maintenance of passive and Active Range of Motion (R.O.M) :
- The patient’s lower limb should be moved passively by the therapist through full range of motion if the patient is not able to perform the active movement.
- If the patient is able to perform the active movement, therapist should encourage it.
- Passive movements need to be given every two hourly hence the patient’s relative should be taught about it.
- Advantage of passive movement exercise :
- Help to maintain the properties of the muscles.
- Prevent tightness and contracture.
- Maintain the normal physiological length of soft tissues.
- Maintain the memory of the movement pattern in the brain which may help in later stages of recovery.
- Help in reducing spasticity if given in a gentle, slow and rhythmic manner.
Maintenance of good Bronchial Hygiene :

- Proper lung hygiene should be maintained by given proper positioning, nebulization, and regular suctioning.
- If the patient is not on ventilatory support then he should be taught breathing exercises and encouraged doing it every hour.
Care of Skin :
Due to constant immobilization patient can develop pressure sores at certain part of body like, sacrum, heel, lateral side of the knee, occiput, etc.
- Prevention of pressure sores is achieved by undertaking the following measures :
- The patient’s attendant and nursing staff should be advised to keep changing the position of the patient every 2 hourly.
- Good skin hygiene is maintained by given regular sponge bath and applying talcum powder.
- Bed linen is kept dry and free of creases.
- Beds that bring about a more uniform distribution of body weight should be given, waterbed or airbed is used.
- Gently massaging the pressure susceptible areas also increases the circulation in that area preventing the chances of infection.
- If pressure sores do develop then it should be treated at the early stage and wound should be prevented from getting infected so that the rate of healing is faster. This can be achieved by the following :
- Regular dressing of wound.
- Cryotherapy around the wound to increase circulation.
- Infrared therapy over the wound also increase blood supply to the part and help in faster recovery.
- If the wound is infected then UVR can be given.
- LASER therapy at appropriate dose can be very effective in healing the pressure sores.
- Direct current given at the edges of the sores help in healing.
Care of Bladder :
- The patient is taught self-cleaning techniques and intermittent catheterization.
- For LMN type of bladder valsalva maneuver is taught.
- For UMN type of bladder intermittent catheterization technique or timed voiding program may be given.
Active Exercise :
- As the patient shows signs of active contraction of muscles and active participation, active cooperation of the patient should be started.
- Active exercise will help the patient to make functionally independent.
- The common exercise consist of : mat exercise,strengthening exercise, weight bearing exercise,gait training and transfer, exercise to normalize the tone.

1) Mat Exercise :
- To prepare the patient for gait training and erect posture mat exercises play a very important role which will make the patient functionally independent.
- The activity consist of turning to each sides, rolling and bridging.
- In prone position the patient may be given activity such as coming on to forearms, coming on to extended forearms, quadripedal position with the help of some external support, kneeling with support, half kneeling,etc.
2)Strengthening Exercise :
- These consist of exercise to strengthen the lower limb muscles.
- Strengthening of the upper limb is also necessary as this will help the patient in transferring, use of walking aids like crutch, etc.
- Strengthening of trunk muscles will help in better balancing in sitting or standing.
- Quadratus lumborum is the most important muscle in case of paraplegia because it enables the patient to hike the pelvis and clear the paretic limb off the ground thus enabling the patient to be ambulant.

3) Use of Tilt Table :
- In the initial stage when there is no trunk stability patient can be trained for weight bearing on lower limbs by using tilt table.
- In this the patient’s trunk and the lower limbs are strapped to the tilt table and then the table is gradually tilted everyday at increasing range so that the autonomous nervous system is made to get conditioned as a result the reflex vasoconstiction can be stimulated in erect position.
- Tilt table can also used to prevent the chances of orthostatic hypotension.
4)Transfer Activities :

- To make the patient independent in ADL, it is necessary to train them to use the wheelchair and transfer from and to wheelchair.
- Easy ways of transfer from bed to wheelchair, from wheelchair to low stool, from low stool to floor, back to wheelchair, various way of locomotion in emergency situation like shuffling in sitting position, semicrawling in prone position with the help of weight bearing on the forearm should be taught to the patient.
5)Gait Training :
- Paraplegic patient can be made to ambulate with the help of crutches and calipers.
- However walking should be trained in a gradual manner.
- The lower limbs are supported with appropriate orthosis and the patient is made to stand in the parallel bar.
- The patient is advised to do hyperextension at the hips and trunk to maintain erect posture and balance which will provide stability.
- Once the patient is confident in standing gait training is started by instructing the patient to lift one leg and take eight on the other extrimity.
- Stepping forward is taught next and the therapist progresses to walking in parallel bars.
- Then patient is made to walkout of the parallel bar with the help of walker.
- Depending on the trunk stability and confidence of the patient progression can be made to axillary crutches.
- Weight bearing on the lower limbs in erect posture also act to slow down the process of osteoporosis and prevent tightness.
6)Use of Orthosis :
- Lower limb orthosis or gaiter may be used depending on the muscular status in the lower limbs like Ankle foot orthosis, Posterior knee gaurd.
7)Management of Spasticity :
It is always better to keep the spasticity under control. Spasticity in the muscles can be reduced by the following methods :
- Gentle rhythmic passive movement
- Sustained gradual stretching either manually or by using splints
- Prolonged icing over the spastic muscle bulk for about 15 to 20 minutes
- Faradic stimulation to the weak antagonist muscle can reduce the spasticity of the agonist muscle by the principle of reciprocal inhibition
- Reflex inhibiting pattern
- Biofeedback : This can be used to relax spastic muscle and to activate its antagonist.
Social and Economical Rehabilitation :
- The therapist should also aim to provide him with some sort of economical independency so that he feel socially acceptable.
- This is very important in younger individuals who have family members dependent on them.
- Therapist should try to keep the patient’s moral and motivation high during whole process.
- The patient should be provided a job which involves skill of the upper limb like, carvings, embroidery, computer job, etc.
- Therapist should try to keep them engaged so that they no longer keeps thinking about their impairment but focus on a much more positive aspect of life.
- The overall rehabilitation of the patient depend upon their motivation, and determination along with skill, dedication of the therapist.
Prognosis :
- Early death rates after admission for TSCI range from 4 to 20%.The patient’s age, level of spinal cord injury, and neurologic grade predict surviva.
- Severe systemic injuries, traumatic brain injury, and medical comorbidity also increase mortality.
- Compared with spinal cord injuries in the thoracic cord or lower, patients with C1 to C3 injuries have a 6.6-fold increased risk of death, C4 to C5 injuries a 2.5 increased risk, and C6 to C8 a 1.5 increased risk.Survivors of TSCI have a reduced life expectancy as well.
- Rates of motor score improvements are also related to the initial severity and level of injury.
- The greatest degrees of improvement are seen in those with incomplete injury and in those without significant comorbidities or medical complications, such as infection.
Among patients with complete TSCI (ASIA grade A):
- 10 to 15% improve, 3% to ASIA grade D
- Less than 10% will be ambulatory at one year
Among patient with an initial ASIA grade B :
- 54% recover to grade C or D
- 40% regain some ambulatory ability.
Among patients with an initial ASIA grade C and D :
- Independent ambulation is possible for 62 and 97% respectively.
Most recovery in patients with incomplete TSCI takes place in the first six months.