
Shoulder Joint
Shoulder Joint Anatomy
The shoulder joint (or glenohumeral joint from Greek glene, eyeball, + -oid, ‘form of’, + Latin humerus, shoulder) is structurally classified as a synovial ball and socket joint and functionally as a diarthrosis and multiaxial joint. It involves articulation between the glenoid cavity of the scapula (shoulder blade) and the head of the humerus (upper arm bone).
Due to the very loose joint capsule that gives a limited interface of the humerus and scapula, it is the most mobile joint of the human body.
There are four joints making up the ‘shoulder joint’:
- The shoulder joint itself known as the Glenohumeral joint, (is a ball and socket articulation between the head of the humerus and the glenoid cavity of the scapula)
- The acromioclavicular (AC) joint (where the clavicle meets the acromion of the scapula)
- The sternoclavicular (SC) joint (where the clavicle meets the chest bone [sternum])
- The scapulothoracic joint (where the scapula meets with the ribs at the back of the chest)
Introduction
The glenohumeral, or shoulder, joint is a synovial joint that attaches the upper limb to the axial skeleton. It is a ball-and-socket joint, formed between the glenoid fossa of scapula (gleno-) and the head of humerus (-humeral).
Acting in conjunction with the pectoral girdle, the shoulder joint allows for a wide range of motion at the upper limb; flexion, extension, abduction, adduction, external/lateral rotation, interna/medial rotation and circumduction. In fact, it is the most mobile joint of the human body. This shoulder function comes at the cost of stability however, as the bony surfaces offer little support. Instead, the surrounding shoulder muscles and ligamentous structures offer joint security; the capsule, ligaments, and tendons of the rotator cuff muscles. Because of this mobility-stability compromise, the shoulder joint is one of the most frequently injured joints of the body.
Introduction of shoulder joint in brief
| Type | Synovial Ball and socket type of joint; multiaxial |
| Articulating surface | Glenoid fossa of scapula, head of humerus; glenoid labrum |
| Ligaments | Superior glenohumeral, middle glenohumeral, inferior glen-ohumeral, coracohumeral, transverse humeral |
| Innervation | Subscapular nerve (joint); suprascapular nerve, axillary nerve, lateral pectoral nerve (joint capsule) |
| Blood supply | Anterior and posterior circumflex humeral, circumflex scapular and suprascapular arteries |
| Movements | Flexion, extension, abduction, adduction, external/lateral rotation, internal/medial rotation and circumduction |
| Rotator cuff muscles | Supraspinatus, infraspinatus, teres minor, subscapularis Mnemonic: Rotator cuff SITS on the shoulder |
Bones & Joints of the Shoulder
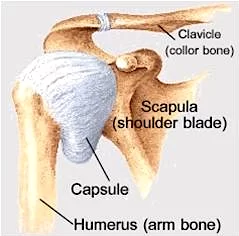
The bones of the shoulder consist of the humerus (the upper arm bone), the scapula (the shoulder blade), and the clavicle (the collar bone).
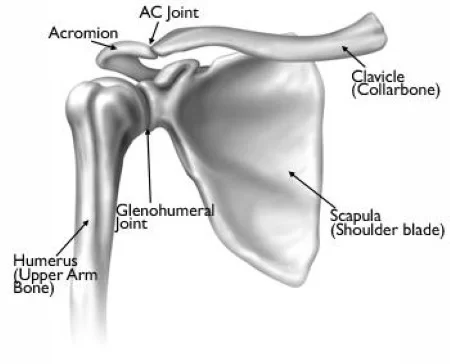
The clavicle is the only bony attachment between the trunk and the upper limb. It forms the front portion of the shoulder girdle and is palpable along its entire length with a gentle S-shaped contour.The clavicle articulates at one end with the sternum (chest bone) and with the acromion of the scapula at the other. This articulation between the acromial end of the clavicle and the acromion of the scapula forms the roof of the shoulder.
The scapula is a large, flat triangular bone with three processes called the acromion, spine and coracoid process . It forms the back portion of the shoulder girdle. The spine (which is located at the back of the scapula) and the acromion can be readily palpated on a patient.
The flat blade of the scapula glides along the back of the chest allowing for extended movement of the arm. The coracoid process is a thick curved structure that projects from the scapula and is the attachment point of ligaments and muscles.
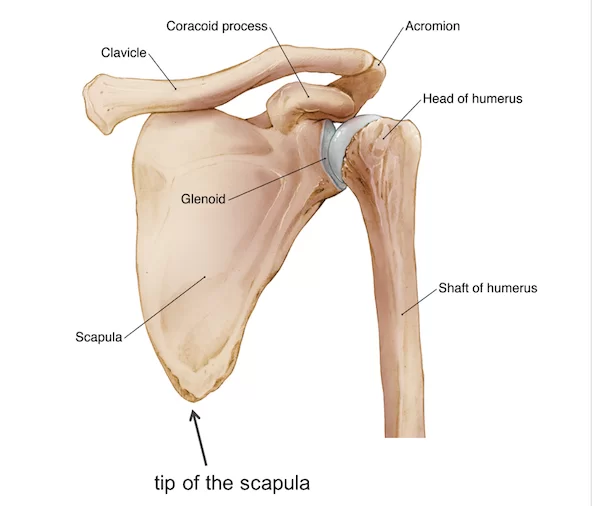
The scapula is also marked by a shallow, somewhat comma-shaped glenoid cavity, which articulates with the head of the humerus.
The top end of the humerus consists of the head, the neck, the greater and lesser tubercles, and the shaft. The head is half-spherical in shape and projects into the glenoid cavity. The neck lies between the head and the greater and lesser tubercles. The greater and lesser tubercles are prominent landmarks on the humerus and serve as attachment sites for the rotator cuff muscles.
Structures of the Shoulder Joint
Articulating Surfaces
The shoulder joint is formed by the articulation of the head of the humerus with the glenoid cavity (or fossa) of the scapula. This gives rise to the alternate name for the shoulder joint – the glenohumeral joint.
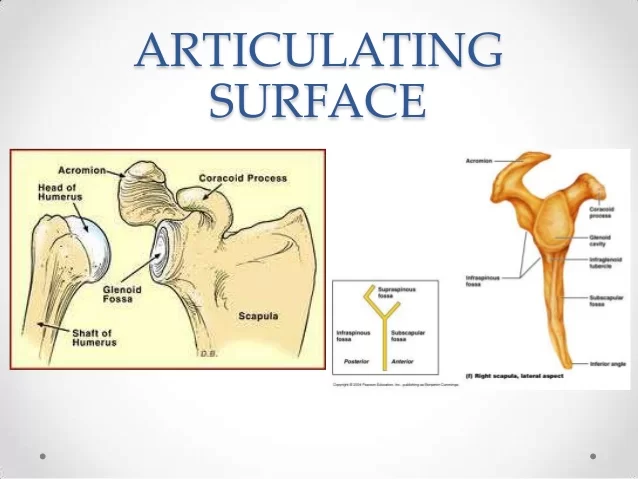
Like most synovial joints, the articulating surfaces are covered with hyaline cartilage. The head of the humerus is much larger than the glenoid fossa, giving the joint a wide range of movement at the cost of inherent instability. To reduce the disproportion in surfaces, the glenoid fossa is deepened by a fibrocartilage rim, called the glenoid labrum.
The glenoid fossa is a shallow pear-shaped pit on the superolateral angle of scapula. The concavity of the fossa is less acute than the convexity of the humeral head, meaning that the articular surfaces are not fully congruent. Congruency is increased somewhat by the presence of a glenoid labrum, a fibrocartilaginous ring that attaches to the margins of the fossa. The labrum acts to deepen the glenoid fossa slightly, it is triangular in shape and thicker anteriorly than inferiorly. The surface of the humeral head is three to four times larger than the surface of glenoid fossa, meaning that only a third of the humeral head is ever in contact with the fossa and labrum.
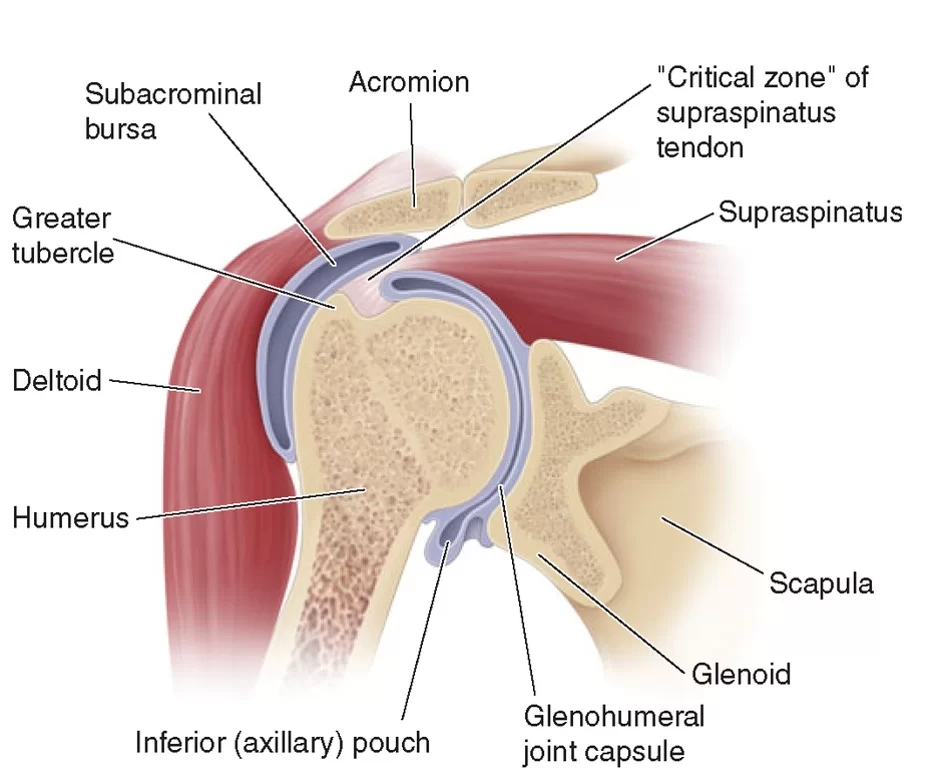
Joint capsule
The shoulder joint is encircled by a loose fibrous capsule. It extends from the scapula to the humerus, enclosing the joint on all sides. The internal surface of the capsule is lined by a synovial membrane.
On the humerus, the capsule attaches to its anatomical neck. Extending only at its medial margin, where the fibers protrude by around 1 cm. On the scapula, the capsule has two lines of attachments. The first is on its anterior and inferior sides where the capsule inserts into the scapular neck, posterior to the glenoid labrum. The second is on its superior and posterior aspects, where the capsular fibers blend directly with the glenoid labrum. Here the capsule arches over the supraglenoid tubercle and it’s long head of biceps brachii muscle attachment, thus making these intra-articular structures.
The capsule remains lax to allow for mobility of the upper limb. It relies on ligaments and muscle tendons to provide reinforcement. The anterior capsule is thickened by the three glenohumeral ligaments while the tendons of the rotator cuff muscles spread over the capsule blending with its external surface. These tendons form a continuous covering called the rotator capsule. It is comprised of the supraspinatus superiorly, infraspinatus and teres minor posteriorly, subscapularis anteriorly, and the long head of triceps brachii inferiorly.
Two weak spots exist in this reinforced capsule. The first is the rotator interval, an area of an unreinforced capsule that exists between the subscapularis and supraspinatus tendons. The second is the inferior capsular aspect, this is the point where the capsule is the weakest. The loose inferior capsule forms a fold when the arm is in the anatomical position. It becomes stretched, and least supported when the arm is abducted.
The capsule has two openings;
- Between the greater and lesser tubercles of the humerus, through which the tendon of the long head of the biceps brachii passes.
- Between the superior and middle glenohumeral ligaments, via which the subscapular bursa communicates with the glenohumeral joint cavity.
Bursa at the shoulder joint
To reduce friction in the shoulder joint, several synovial bursae are present. A bursa is a synovial fluid-filled sac, which acts as a cushion between tendons and other joint structures.
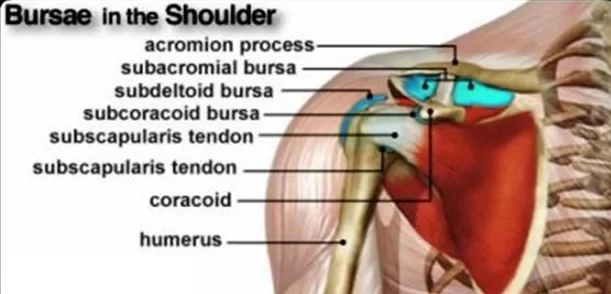
The bursae that are important clinically are:
Synovial fluid-filled bursae assist with the joint’s mobility.
- The subdeltoid-subacromial (SASD) bursa is located between the joint capsule and the deltoid muscle or acromion, respectively. and superficial to the supraspinatus tendon and joint capsule. The subacromial bursa reduces friction beneath the deltoid, promoting free motion of the rotator cuff tendons. Subacromial bursitis (i.e. inflammation of the bursa) can be a cause of shoulder pain.
- The subcoracoid bursae are found between the capsule and the coracoid process of the scapula.
- The coracobrachial bursa is located between the subscapularis and coracobrachialis muscles. These bursae allow the structures of the shoulder joint to slide easily over one another.
- Subscapular – located between the subscapularis tendon and the scapula. It reduces wear and tear on the tendon during movement at the shoulder joint.
Shoulder labrum
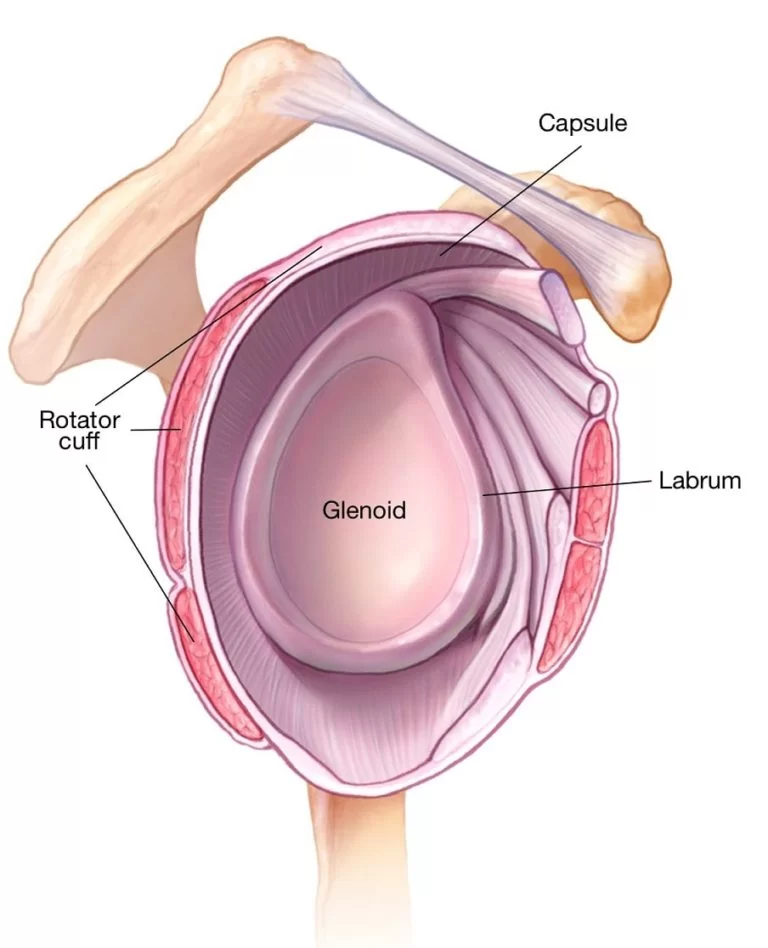
The labrum is a slippery, tough ring of cartilage that rims the glenoid cavity (shoulder socket). The labrum helps:
- Keep the head of the humerus in place
- Ensure smooth movement of the ball-and-socket joint
- A shoulder’s labrum can be damaged or torn as a result of an acute injury, overuse, or as part of the aging process.
Ligaments of shoulder
Several ligaments limit the movement of the GH joint and resist humeral dislocation. These are the coracohumeral, glenohumeral and transverse humeral ligaments. Glenohumeral and transverse humeral are capsular ligaments while coracohumeral is an accessory ligament.
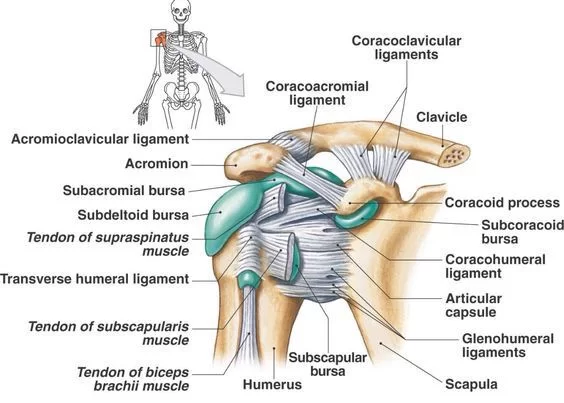
The transverse humeral ligament extends horizontally between the tubercles of the humerus. It covers the intertubercular sulcus and the long head tendon of the biceps brachii muscle, preventing displacement of the tendon from the sulcus. The coracohumeral ligament (Ligamentum coracohumerale) extends between the coracoid process of the scapula to the tubercles of the humerus and the intervening transverse humeral ligament, supporting the joint from its superior side. It acts to limit inferior translation and excessive external rotation of the humerus.
The superior, middle and inferior glenohumeral ligaments support the joint from the anteroinferior side. They have a weak stabilizing function, each acting to limit the maximum amplitude of certain arm movements;
All three ligaments become taut during external (lateral) rotation of humerus, while they relax in internal (medial) rotation. They also resist anterior translation of the humeral head.
The middle and inferior ligaments tense during abduction, while the superior is relaxed.
The superior glenohumeral ligament extends from the supraglenoid tubercle of scapula to the proximal aspect of the lesser tubercle of humerus. Along with the coracohumeral ligament, it supports the rotator interval and prevents inferior translation of the humeral head, particularly during shoulder adduction.
The middle glenohumeral ligament attaches along the anterior glenoid margin of the scapula, just inferior to the superior GH ligament. It extends to the lesser tubercle of humerus. This wide ligament lies deep to, and blends, with the tendon of subscapularis muscle. It stabilizes the anterior capsule, limiting external rotation, particularly when the arm is in an abducted position (45o – 60o abduction).
The inferior glenohumeral ligament is a sling-like ligament extending between the glenoid labrum and the inferomedial part of the humeral neck. It is split into anterior and posterior bands, between which sits the axillary pouch. This is the strongest of the three GH ligaments, being thicker and longer than the other two. Both bands stabilize the humeral head when the arm is abducted above 90°. The anterior band limits external rotation of the arm, while the posterior band limits internal rotation.
Coraco–clavicular ligament – composed of the trapezoid and conoid ligaments and runs from the clavicle to the coracoid process of the scapula. They work alongside the acromioclavicular ligament to maintain the alignment of the clavicle in relation to the scapula. They have significant strength but large forces (e.g. after a high energy fall) can rupture these ligaments as part of an acromio-clavicular joint (ACJ) injury. In severe ACJ injury, the coraco-clavicular ligaments may require surgical repair.
The other major ligament is the coracoacromial ligament. Running between the acromion and coracoid process of the scapula it forms the coraco-acromial arch. This structure overlies the shoulder joint, preventing superior displacement of the humeral head.
Movements of the shoulder joint
Being a ball-and-socket joint, it allows movements in three degrees of freedom (average maximum glenohumeral active RoM is shown in brackets);
- Flexion (180°) – extension (60°)
- Abduction (180°) – adduction (40°)
- Internal rotation (90°) – external rotation (90°)
Combination of these movements gives circumduction.
Activities of the arm rely on movement from not only the glenohumeral joint but also the scapulothoracic joint (acromioclavicular, sternoclavicular and scapulothoracic articulations). Together these joints can change the position of the glenoid fossa, relative to the chest wall. Thus repositioning the glenohumeral joint, and upper limb, within space. This provides for a greater range of motion available within the greater shoulder complex;
Flexion (180°) – extension (90°)
Abduction (180°) – adduction (30°)
Internal rotation (90°) – External rotation (90°)
The close-packed position of the glenohumeral joint is abduction and external rotation, while open packed (resting) position is abduction (40-50°) with horizontal adduction (30°). The joints’ capsular pattern is external rotation, followed by abduction, internal rotation and flexion. The additional accessory movements of spin, roll and slide (glide) are also available within the glenohumeral joint.
- Extension (upper limb backwards in sagittal plane) – posterior deltoid, latissimus dorsi and teres major.
- Flexion (upper limb forwards in sagittal plane) – pectoralis major, anterior deltoid and coracobrachialis. Biceps brachii weakly assists in forward flexion.
- Abduction (upper limb away from midline in coronal plane):
- The first 0-15 degrees of abduction is produced by the supraspinatus.
- The middle fibres of the deltoid are responsible for the next 15-90 degrees.
- Past 90 degrees, the scapula needs to be rotated to achieve abduction – that is carried out by the trapezius and serratus anterior.
- Adduction (upper limb towards midline in coronal plane) – pectoralis major, latissimus dorsi and teres major.
- Internal rotation (rotation towards the midline, so that the thumb is pointing medially) – subscapularis, pectoralis major, latissimus dorsi, teres major and anterior deltoid.
- External rotation (rotation away from the midline, so that the thumb is pointing laterally) – infraspinatus and teres minor.
Mobility and Stability
The shoulder joint is one of the most mobile in the body, at the expense of stability. Here, we shall consider the factors the permit movement, and those that contribute towards joint structure.
Factors that contribute to mobility:
- Type of joint – ball and socket joint.
- Bony surfaces – shallow glenoid cavity and large humeral head – there is a 1:4 disproportion in surfaces. A commonly used analogy is the golf ball and tee.
- Inherent laxity of the joint capsule.
Factors that contribute to stability:
- Rotator cuff muscles – surround the shoulder joint, attaching to the tuberosities of the humerus, whilst also fusing with the joint capsule. The resting tone of these muscles act to compress the humeral head into the glenoid cavity.
- Glenoid labrum – a fibrocartilaginous ridge surrounding the glenoid cavity. It deepens the cavity and creates a seal with the head of humerus, reducing the risk of dislocation.
- Ligaments – act to reinforce the joint capsule, and form the coraco-acromial arch.
- Biceps tendon – it acts as a minor humeral head depressor, thereby contributing to stability.
Innervation
Axillary nerve (Nervus axillaris)
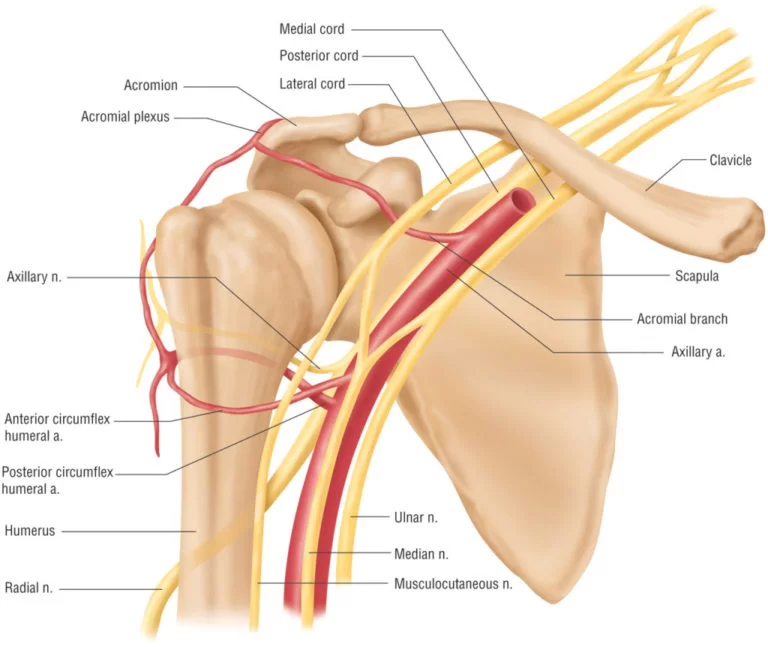
The glenohumeral joint is innervated by the subscapular nerve (C5-C6), a branch of the posterior cord of brachial plexus. The joint capsule is supplied from several sources;
- the suprascapular nerve supplies the posterior and superior aspects
- axillary nerve innervates the anteroinferior part of the capsule
- The lateral pectoral nerve supplies the anterosuperior part and the rotator capsule
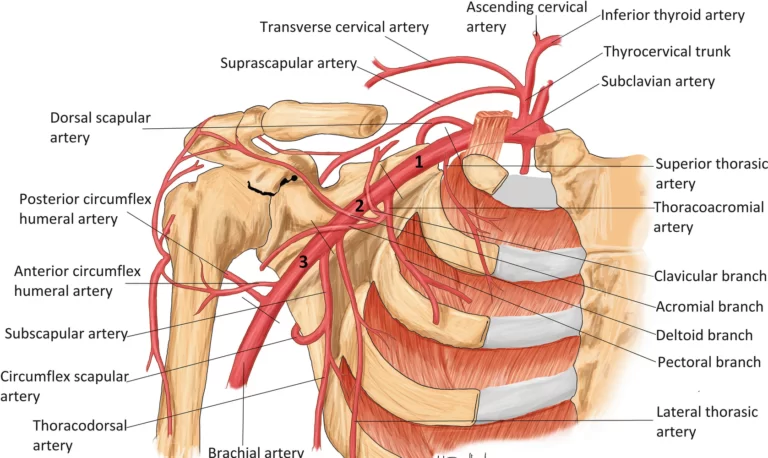
Blood supply
Blood supply to the shoulder joint comes from the anterior and posterior circumflex humeral, circumflex scapular, and suprascapular arteries.
Rotator cuff
Supraspinatus muscle (Musculus supraspinatus)
The rotator cuff muscles are four muscles that form a musculotendinous unit around the shoulder joint. These are the supraspinatus, infraspinatus, teres minor and subscapularis muscles. The function of this entire muscular apparatus is to produce movement at the shoulder joint while keeping the head of humerus stable and centralized within the glenoid cavity.
Rotator cuff Sits on the shoulder
- Supraspinatus
- Infraspinatus
- Teres minor
- Subscapularis
All four muscles are firmly attached around the joint in such a way that they form a sleeve (rotator capsule). Individually, each muscle has its own pulling axis that results in a certain movement (prime mover), while together they create a concavity compression. This is a stabilizing mechanism in which compression of the humerus into the concavity of glenoid fossa prevents its dislocation by translating forces.
Pathology of Shoulder joint
- Frozen shoulder: Inflammation develops in the shoulder that causes pain and stiffness. As a frozen shoulder progresses, movement in the shoulder can be severely limited.
- Osteoarthritis: The common “wear-and-tear” arthritis that occurs with aging. The shoulder is less often affected by osteoarthritis than the knee.
- Rheumatoid arthritis: A form of arthritis in which the immune system attacks the joints, causing inflammation and pain. Rheumatoid arthritis can affect any joint, including the shoulder.
- Gout: A form of arthritis in which crystals form in the joints, causing inflammation and pain. The shoulder is an uncommon location for gout.
- Rotator cuff tear: A tear in one of the muscles or tendons surrounding the top of the humerus. A rotator cuff tear may be a sudden injury, or result from steady overuse.
- Shoulder impingement: The acromion (edge of the scapula) presses on the rotator cuff as the arm is lifted. If inflammation or an injury in the rotator cuff is present, this impingement causes pain.
- Shoulder dislocation: The humerus or one of the other bones in the shoulder slips out of position. Raising the arm causes pain and a “popping” sensation if the shoulder is dislocated.
- Shoulder tendonitis: Inflammation of one of the tendons in the shoulder’s rotator cuff.
- Shoulder bursitis: Inflammation of the bursa, the small sac of fluid that rests over the rotator cuff tendons. Pain with overhead activities or pressure on the upper, outer arm are symptoms.
- Labral tear: An accident or overuse can cause a tear in the labrum, the cuff of cartilage that overlies the head of the humerus. Most labral tears heal without requiring surgery.
Shoulder Tests
- Magnetic resonance imaging (MRI scan): An MRI scanner uses a high-powered magnet and a computer to create high-resolution images of the shoulder and surrounding structures.
- Computed tomography (CT scan): A CT scanner takes multiple X-rays, and a computer creates detailed images of the shoulder.
- Shoulder X-ray: A plain X-ray film of the shoulder may show dislocation, osteoarthritis or a fracture of the humerus. X-ray films cannot diagnose muscle or tendon injuries.
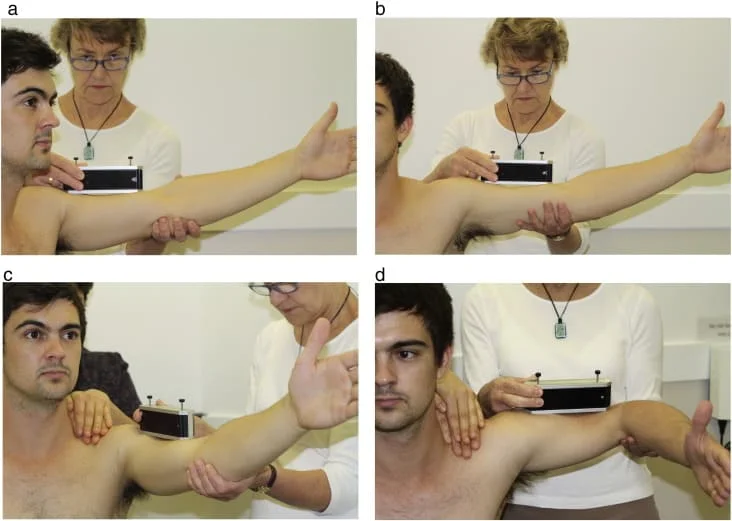
Shoulder Special Tests
Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803


53 Comments