
TECHNIQUES TO INHIBIT SPASTICITY WITH PHYSIOTHERAPY TREATMENTS
SPASTICITY OF Muscles :
DEFINITION:
- Spasticity of Muscles is a feature of altered skeletal muscle performance with a combination of paralysis, increased tendon reflex activity and hypertonia.
- It is also colloquially referred to as an unusual “tightness”, stiffness, or “pull” of muscles.
Functional definition: The abnormal motor control caused by an UMN lesion (as in spastic paraparesis).
UPPER MOTOR NEURON SYNDROME:
Positive Signs:
- Spasticity
- Rigidity
- Hyperreflexia
- Primitive reflexes
- Clonus
Negative Signs:
- Lack of strength
- Lack of motor control
- Lack of coordination
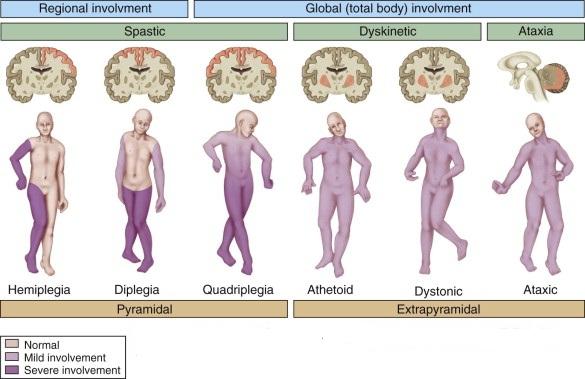
EXAMPLE OF UPPER MOTOR NEURON DISEASE:
- Stroke
- Multiple Sclerosis
- Cortico basal Ganglionic Degeneration
- Traumatic Brain Injury
- Acquired Brain Injury
- Spinal Cord Injury
- Cerebral Palsy
CAUSES OF SPASTICITY:
- Spasticity is caused by an imbalance of signals from the central nervous system (brain and spinal cord) to the muscles.
- This imbalance is often found in people with cerebral palsy, traumatic brain injury, stroke, multiple sclerosis, and spinal cord injury.
SIGNS AND SYMPTOMS OF SPASTICITY:
- Increased muscle tone.
- Overactive reflexes.
- Involuntary movements, which may include spasms (brisk and/or sustained involuntary muscle contraction) and clonus (series of fast involuntary contractions).
- Pain and discomfort.
- Decreased functional abilities and delayed motor development.
- Difficulty with care and hygiene.
- Abnormal posture.
- Contractures (permanent contraction of the muscle and tendon due to severe persistent stiffness and spasms).
- Bone and joint deformities.
- Skin breakdown-shear.
- Interferes with breathing.
- Hampers gait and transfer.
- More work for caregiver.
- Poor safety.
- Sexual difficulties.
- Insomnia.
- Poor posture.
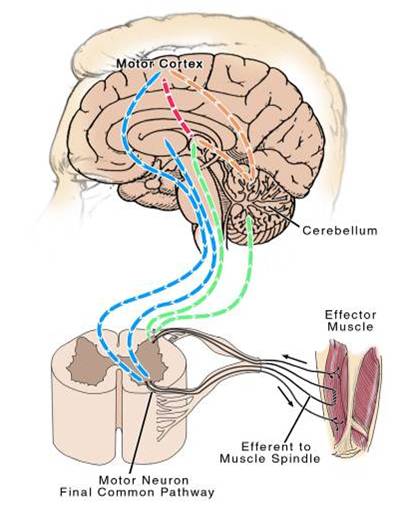
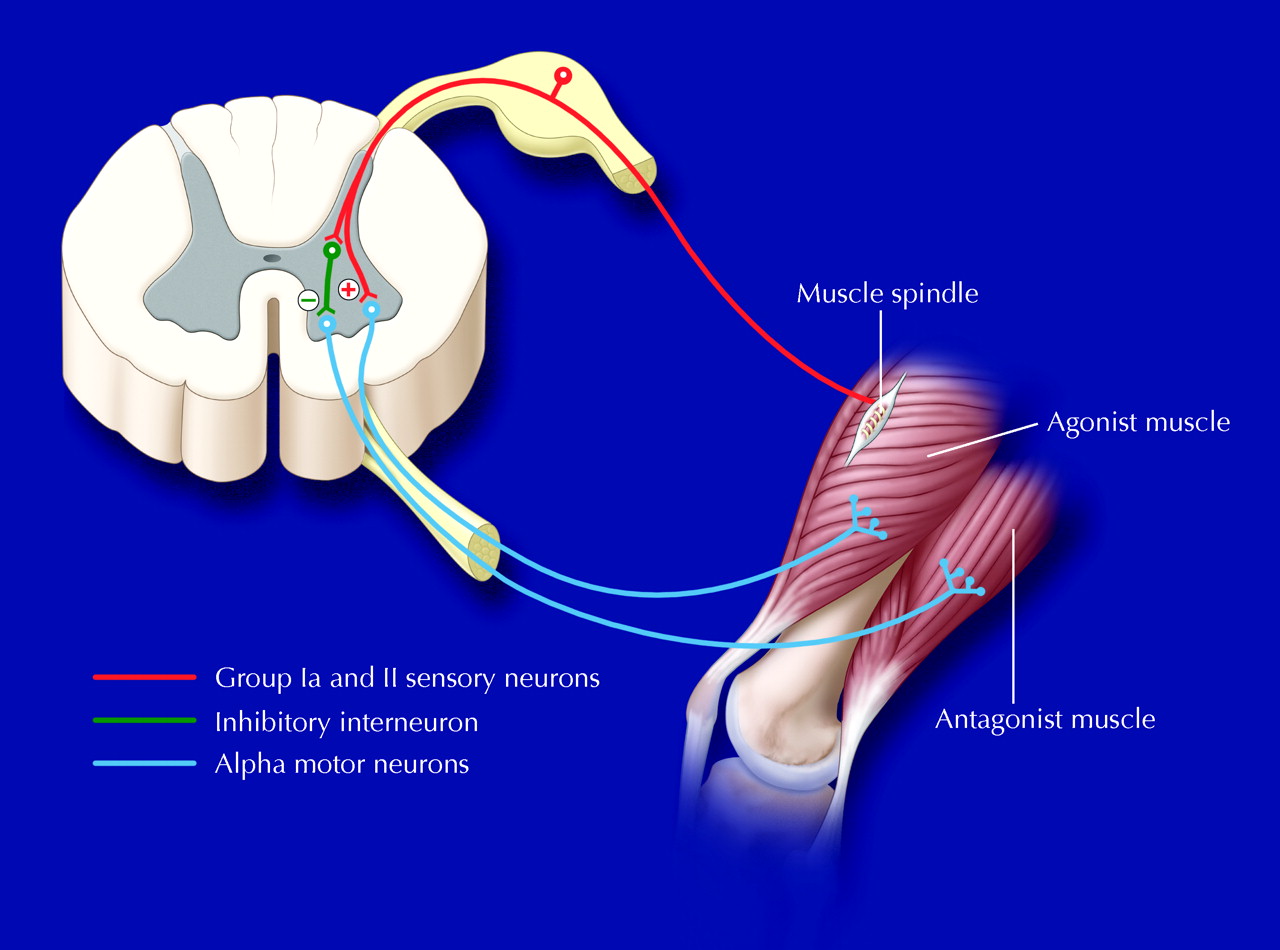
PATHOPHYSIOLOGY OF SPASTICITY OF MUSCLES :

SPASTICITY ASSESSMENT:
- Patient report.
- Deep tendon reflexes.
- Passive range of motion.
- Test for clonus.
- Functional observation:
- Determine nature of hypertonicity
- Assess interference with function (gait) and effect of stress and/or fatigue
- Assess adaptive shortening of muscles vs. irreversible contracture
- Consider aggravating factors. (e.g., UTI, infection, excessive activity, strengthening exercises)
MODIFIED ASHWARTH SCALE:
- DEFINITION:
The Modified Ashworth scale (MAS) measures resistance during passive soft-tissue stretching and is used as a simple measure of spasticity.
INSTRUCTION:
- Place the patient in a supine position.
- If testing a muscle that primarily flexes a joint, place the joint in a maximally flexed position and move to a position of maximal extension over one second (count “one thousand one”).
- If testing a muscle that primarily extends a joint, place the joint in a maximally extended position and move to a position of maximal flexion over one second (count “one thousand one”)
- Score based on the classification below
Scoring of modified Ashwarth scale:
- 0 No increase in muscle tone
- 1 Slight increase in muscle tone, manifested by a catch and release or by minimal resistance at the end of the range of motion when the affected part(s) is moved in flexion or extension.
- 1+ Slight increase in muscle tone, manifested by a catch, followed by minimal resistance throughout the remainder (less than half) of the ROM.
- 2 More marked increase in muscle tone through most of the ROM, but affected part(s) easily moved.
- 3 Considerable increase in muscle tone, passive movement difficult.
- 4 Affected part(s) rigid in flexion or extension.
Spasticity Treatment :
CONSIDERATIONS IN REDUCING SPASTICITY OF MUSCLES :
Possible advantages of spasticity :
- Maintains muscle tone/bulk.
- Helps support circulatory function.
- May prevent formation of deep vein blood thrombosis.
- May assist in activities of daily living.
- May assist with postural control.
Spasticity Physiotherapy treatment & Exercise :
SPASTICITY REHABILITATION INTERVENTION:


- Static stretch.
- Gait training (emphasis on swing and heel strike).
- Positioning/posture.
- Cooling.
- Patient education.
- Relaxation.
- Bio-feedback: These techniques involve monitoring muscle activity via a device that records when a spastic muscle relaxes or contracts.
- Facilitation: This includes neurodevelopmental therapy (also known as Bobath approach) aimed at reducing inappropriate reflexes and training your muscles to achieve normal balanced reactions. Proprioceptive neuromuscular facilitation seeks to retrain spastic muscles for normal motion. Sensory integration involves continually repeating tasks, often with the therapist directing the limb while you remain passive, so that your brain is “retrained” in the proper movements.
- Reflex-inhibiting movement patterns.
- Avoiding noxious stimuli.
- Medications.
- ITB Therapy.
- Botulinum Toxin.
SPASTICITY MEDICAl TREATMENT:
Baclofen (Lioresal)
- GABA agonist
- Max. dose 180 mg daily, divided
- Side effects: sedation, incontinence, weakness, withdrawal seizures
Tizanidine (Zanaflex)
- Alpha2 adrenergic agonist
- Max. dose 24-32 mg daily
- Side effects: sedation, hypotension, weakness, hepatotoxicity
Dantrolene – reserve for specialists
Diazepam et al. (Valium)
Gabapentin (Neurontin)
SPASTICITY INVASIVE TREATMENTS:
- Botulinum Toxins A & B
- Baclofen pump
- Intrathecal delivery via implanted pump (ITB)
- Surgical interventions:
Tenotomy (Tendon Lengthening)
Selective Rhizotomy
PHYSIOTHERAPY FOR SPASTICITY CONTROL:
- Reduction of noxious stimulation.
- Positional Stretching and weight bearing Activity.
- Muscle Long Stretching.
- Physical modalities like, Cooling- Icing, Heat.
- Electrical stimulation: Electrical stimulation is sometimes used to re-educate muscles, usually with the goal of resetting the balance between your flexor and extensor muscles. The effects usually last for about 10 minutes when the stimulation is first applied, but after several months the effects may become longer lasting.
Muscle strengthening. - Orthoses: Also known as casts, braces, or splints, orthoses include any device that is used to support, align, prevent, or correct deformities or improve the function of movable parts of the body. When used to treat spasticity, orthoses may reduce muscle tone, increase or maintain motion, and prevent skin damage such as the breakdown that would occurs in your palm if your fist is continually clenched.
Other Related Article :


Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803




Is swimming and weight bearing increase spasticity ?
In spasticity the muscle tone is already increased . You recommend weight bearing which may increase it even further ?
swimming and weight bearing activity reduced spasticity and strengthen other opposite group muscle and improve overall joint movement cotrol. swimming is not able to do movement in patient in early stages but weight bearing activity patient can started gradually in early stages.