
Brachioradialis muscle Anatomy, Origin, Insertion, Function
Introduction
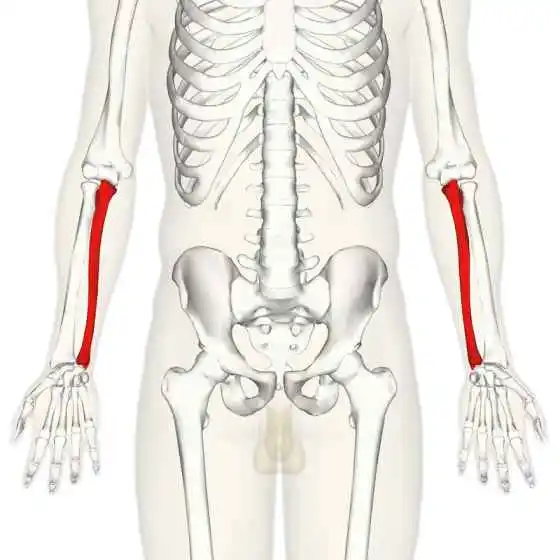
The brachioradialis or also known as supinator longus is a superficial muscle located in the outer aspect of the back of the forearm. It is a fusiform muscle. In other words, the brachioradialis has two tendons at the origin and insertion and has got a muscle belly in between. Technically although brachioradialis forms the part of the superficial layer of the posterior compartment of the forearm muscle along with extensor carpi radialis brevis and extensor carpi radialis longus, it is visible from the anterior compartment.
The brachioradialis muscle has distinctive origin and insertion points as compared to other muscles. It arises from the distal end of the humerus and ends in the distal end of the radius.
Origin of the Brachioradialis Muscle
The brachioradialis is proximally attached to the upper two-thirds of the lateral supracondylar ridge of the humerus and the anterior surface of the lateral intramuscular septum of the arm. The muscle then courses downwards to the outer side of the forearm and crosses over to the cubital fossa or the groove at the elbow joint.
Insertion of the Brachioradialis Muscle
The muscle belly courses downwards along the lateral side of the front of the forearm only to tapper at the end and form a thick tendon which further continues its journey and inserts itself just proximal to the styloid process of the radius, to the lateral side of the radial bone.
Nerve Supply
The Brachioradialis is a muscle in the posterior compartment of the forearm, and just like all the muscles of the posterior compartment is supplied by the radial nerve.
Though radial nerve roots are C5, C6, C7, C8, and sometimes to T1, the brachioradialis muscle is primarily innervated by the C5 and C6 nerve roots.
Blood Supply
The brachioradialis muscle is supplied by the recurrent radial artery, a branch of the radial artery. It runs below the elbow joint, from distal to proximal, and takes part in the collateral circulation of the elbow joint.
The brachioradialis has two venous drainages, superficial and deep. The median cubital vein completes the superficial venous drainage in the lateral forearm which is a branch of the cephalic vein, along with the basilic vein which runs along the medial forearm. The deep venous drainage is done by the paired vessels around the named arteries of the forearm.
The Function of the Brachioradialis Muscle
The human forearm is divided into five compartments including
- the volar superficial
- the volar deep
- the dorsal superficial
- the dorsal deep
- the mobile wad
The brachioradialis along with the extensor carpi radialis longus and extensor carpi radialis brevis muscles forms the mobile wad. The mobile wad or the Wad of Henry is located in the lateral compartment of the forearm and consists of all the muscles responsible for the flexors of the elbow joint.
The brachioradialis, though belonging to the posterior compartment of the forearm is a flexor rather than an extensor. It is the chief flexor of the elbow joint. The muscle is active during elbow flexion whether the forearm is supinated, neutral, or pronated.
An EMG study by Michael R. Boland showed that while the neutral position of the forearm is thought to result in the strongest brachioradialis force, the greatest EMG activation of the brachioradialis occurs during every elbow flexion regardless of the forearm position.
Anatomically, the muscles exert the strongest force when the fibers are aligned parallel to each other. This gives the idea that the brachioradialis will exhibit its maximal force when the arm is in the mid-prone position, i.e when the palm is perpendicular to the ground. This is what anatomists consider might be the reason why the brachioradialis muscle is the muscle of choice while lifting weights or performing activities from the mid-prone position. They include picking up things like water bottles, carrying bags, rowing, hammering, or doing craftsman work.
The brachioradialis has a role in supination and pronation of the forearm. Anatomically, brachioradialis will bring back the hand to a semi-prone position despite if it is supinated or pronated.
A study was conducted recording the EMG activity of the brachioradialis muscle during rotational tasks. It was concluded that more activation is seen while the muscle performs pronation as compared to supination. This led a few to conclude that the brachioradialis is more of a pronator than the supinator.
Since brachioradialis crosses over the elbow joint, it plays a significant role in stabilizing the elbow during repetitive eccentric contractions like lifting weights.
Palpation of the Brachioradialis Muscle
The brachioradialis, though the muscle of the posterior compartment is palpated along the lateral aspect of the anterior side of the forearm.
- To palpate the muscle, make the subject sit on a chair or stool.
- Once comfortably sat, ask the patient to rotate their forearm in the mid-prone position, with the elbow perpendicular to the ground
- The examiner places their hand along the lateral condyle of the humerus and goes up to the supracondylar ridge.
- Ask the subject to make little pulses of motion by flexing the elbow from the mid-prone position.
- Once the subject starts the pulsing motion, the examiner slowly brings down the hand and feels the contraction of the brachioradialis muscle.
- The contraction is felt stronger along the muscle belly in the forearm.
Clinical Relevance of the Brachioradialis Muscle
To Test C6 Spinal Nerve
Brachioradialis reflex is done to test the C6 nerve root of the radial nerve.
To perform the reflex test,
- Ask the person to sit in high sitting with the arm to be tested resting on their lap
- Expose the area of the forearm and elbow. Make sure the patient’s clothing is loose and not causing any hindrance in reflex testing.
- The examiner is standing either to the side of the arm or in front of the patient.
- Ask the patient to be as comfortable as possible and relax all the muscles of the body.
- Without their knowledge, strike the reflex hammer about 10 cm above the wrist.
- Please note not to perform the reflex test more than 3-5 times in a setting as it may change the response.
The normal response is slight elbow flexion along with either supination or pronation. Please note no wrist component is involved with brachioradialis reflex testing.
In the case of pathologies, one might find an exaggerated response or no response to an unusual response. For example, in cases of C6 spinal nerve compression, inverted radial reflex or inverted supinator sign is seen. That is, stimulating the brachioradialis tendon produces finger flexion of the same side of the body being tested.
In Surgical Procedures
While performing the volar approach or Henry approach to treat distal radius fractures, brachioradialis is an important structure to take into consideration.
There are two internervous planes for the Henry approach,
- the distal internervous plane, which is between the brachioradialis and flexor carpi radialis.
- the proximal internervous plane is between the brachioradialis and pronator teres.
In both cases, the radial nerve and median nerve are innervating the muscles. And special attention is needed so as not to damage them. Surgeons prefer to release the brachioradialis to decrease the pressure on the distal radius and facilitated volar plating.
Waternberg syndrome is another pathology where brachioradialis, along with extensor carpi radialis longus is released to decrease the compression of the superficial radial nerve. Waternberg syndrome is associated with pain in the backside of the outer part of the forearm, wrist, and hand.
Post Midshaft Humerus Fractures
Following the midshaft fracture of the humerus, brachioradialis is checked to ensure the integrity of the radial nerve below the fracture site. The Brachiordailis and extensor carpi radialis longus are the first two muscles to be innervated by the radial nerve following its course from the radial groove to the forearm.
Checking brachioradialis gives an insight into whether the radial nerve is damaged or not. And if it had been damaged, it is one of the first muscles to reinnervate followed by the injury. It typically takes 3-5 months for complete recovery.
Associated Pathologies of Brachioradialis Muscle
A lot of conditions might cause functional limitations in the movement of brachioradialis. A few of them include,
Brachioradialis strain:
- A huge force to the forearm or wrist might lead to mild or severe tearing of the brachioradialis muscle, resulting in strain.
- Is usually accompanied by pain and swelling in the forearm.
- Leads to functional impairment and activity limitation.
Brachioradialis tendinitis:
- Occurs due to repetitive movements such as playing tennis or doing handyman works such as nailing or hammering.
- Causes swelling around the forearm along with tenderness.
Forearm weakness from cervical radiculopathy:
- Compression of the nerve from the neck might result in tingling, numbness, and decreased functional capacity of the brachioradialis muscle.
- This might cause hindrance in performing daily activities such as lifting things, drinking fluids from bottles, etc.
Avulsion fracture of the brachioradialis tendon:
- A sudden force to the brachioradialis tendon might result in a damaged or torn tendon.
- When the tendon is broken, it chips away a fragment of radial bone with it. This is termed an avulsion fracture.
- This pain, swelling and bruising of the forearm.
- In some cases nerve is also damaged, causing numbness and tingling in the back side of the arm and hand, and sometimes in the thumb and index finger.
Treatment Options for Brachioradialis Muscle
Injury to Brachiordailais is dealt with first with conservative management and then if failed, with surgical methods. Both of them are followed by a period of physiotherapy which involves Pain management, restoration of functions, and inhibiting activity limitation.
The first and foremost treatment option includes the PRICE protocol. It stands for protection, rest, ice, compression, and elevation. This protocol aids in decreasing the initial pain followed by limiting the swelling.
Heat and Ice
Icing or cold packs are applied on brachioradialis to help minimalize localized swelling, pain, and tenderness. Typically icing or cold packs are used till one week of the injury 3-5 times a day for 10-15 minutes in a single sitting.
Once the swelling has decreased, heat is applied in form of hot packs or towels for 10-15 minutes periodically over 2-3 times a day.
While icing aids in reducing inflammation and pain, heat promotes joint mobility, and circulation and relaxes the muscles. Care should be taken to use the appropriate temperature and for a limited duration while applying the packs so as not to cause frost burns or heat burns.
Typically hot packs are between 38-40 degrees celsius and cold packs between 7-10 degrees celsius. And both are applied for a maximum of 20-25 minutes duration, preferably with breaks every 5-7 minutes.
Trigger Point Release
- As the brachioradialis is a frequently used muscle, there are several trigger points in it.
- Ischemic compression followed by soft tissue release along with friction massage can aid in reducing pain felt trigger point, increase the mobility of the area followed by circulation.
Kinesiology Tape
A certified physiotherapist may perform kinesiology taping for the brachioradialis to,
- reduce pain,
- enhance muscle function, or
- provide rest to the muscle followed by an overuse injury.
After the initial period of pain is over, the physiotherapeutic management then moves on to the restoration of the function.
Brachioradialis Stretch
Stretching the muscle can decrease a bit of pressure and promote relaxation. To stretch the brachioradialis muscle,
- Sit in a comfortable position. IF you wish to stand, then stand with knees relaxed and feet hip-width wide.
- Extend the elbow and intertwine the fingers of both hands.
- Flex the wrist and rotate the arm so the palm is facing outwards.
- Stretch the elbow till you feel a little pull.
- Hold the stretch for 15-30 seconds.
- Repeat 3-5 times.
Stretching is then followed by strengthening which is a long process and takes around 1-2 months.
Brachioradialis Strengthening
There are a variety of ways to strengthen the brachioradialis muscle. Most of them include doing weighted or resistive forearm supination and pronation followed by elbow flexion.
Please note that the strengthening regime is personalized for every individual and it is wise to consult with your physiotherapist or sports therapist before starting any new regime or making any changes to the older one.
But one thing common for all is to understand the basic anatomy of the brachioradialis which we have covered in this article along with a few extra facts.

Author: Yashvi Pansari
Dr. Yashvi Pansari - Physiotherapist in Mobile Physiotherapy clinic, B-01, Jagatnagar Society, Opposite- Shaktidhara society, tollnaka, Bapunagar, Ahmedabad



11 Comments