
Disease | Exercise Detail | Neurological problem | Neurology | Paralysis | Pinched Nerve | REHABILITATION | Spinal Problem
Hirayama Disease: Physiotherapy Treatment
Hirayama Disease is characterized by a slow and progressive weakening of the skeletal muscles. It is a rare disease, and it affects people in their teens and early 20s.
Introduction
- Hirayama disease, a rare neurological disease, is characterized by insidious unilateral or bilateral muscular atrophy and weakness of the forearms and hands, without sensory or pyramidal signs.
- The disease primarily affects men in the second to third decades.
- The disease progresses initially, but spontaneous arrest is known to follow several years after the onset, unlike motor neuron disease with which it is commonly confused.
- Hirayama disease is characterized by focal ischemic changes in the anterior horn cells of the lower cervical cord that result in amyotrophy, which is usually unilateral but may also be bilateral. We describe the characteristic findings of flexion magnetic resonance imaging (MRI) suggestive of Hirayama disease.
Hirayama Disease Define
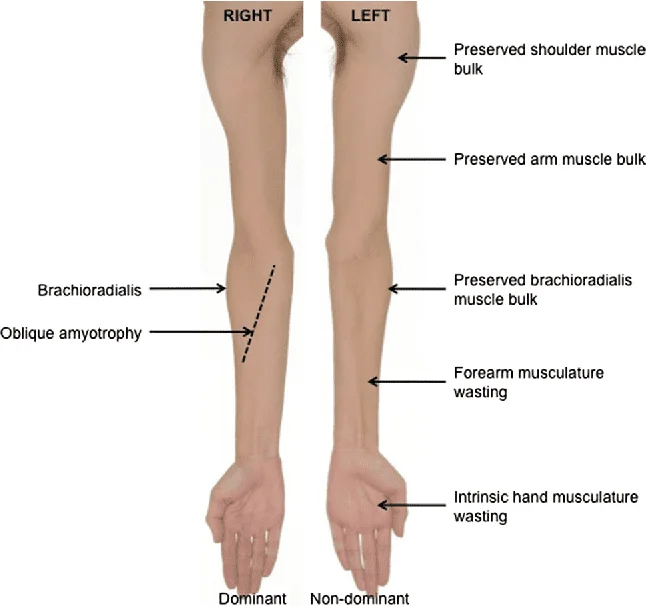
- Also known as monomelic amyotrophy (MMA) is a rare cervical myelopathy that manifests its self as a self -limited asymmetrical ,slowly progressive atrophic weakness of the forearm and hand predominantly in young males.
Monomelic Amyotrophy ( Hirayama Disease )
- MMA is a rare disease that causes muscle weakness in the upper extremities. MMA affects the lower motor neurons. Lower motor neurons are cells that help communicate information from the brain to the muscles that are involved in movement skeletal muscle. Specifically, monomelic amyotrophy causes weakness and loss of muscle mass in the arms and fingers.
- Symptoms of the disease typically begin between the ages of 14-25 years-old. The disease is most common in Asia, especially in Japan and India. Males are more likely to develop the disease than females.
- The exact cause of monomelic amyotrophy is unknown. It is possible that the disease is caused by the movement of the sac that surrounds the spinal cord due to repeated downward movement (flexion) of the neck. Monomelic amyotrophy can sometimes run in families, but it is not thought to be caused by a specific genetic change. Diagnosis of the disease is based on imaging studies and electromyography (EMG) consistent with the disease. Treatment options may include muscle-strengthening exercises and neck bracing.
Pathogenesis
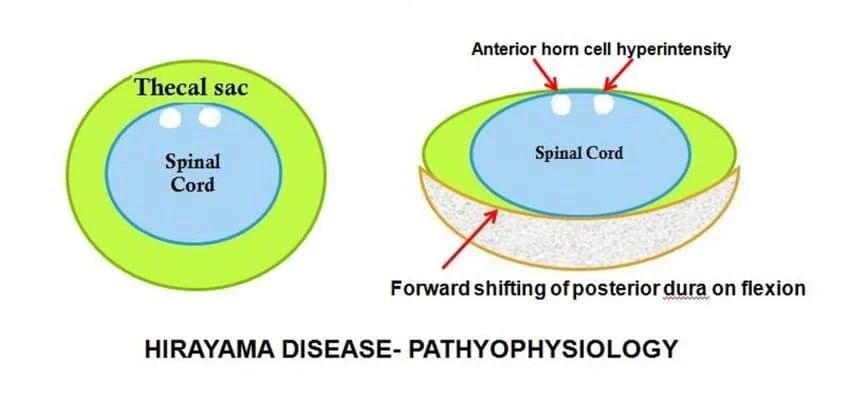
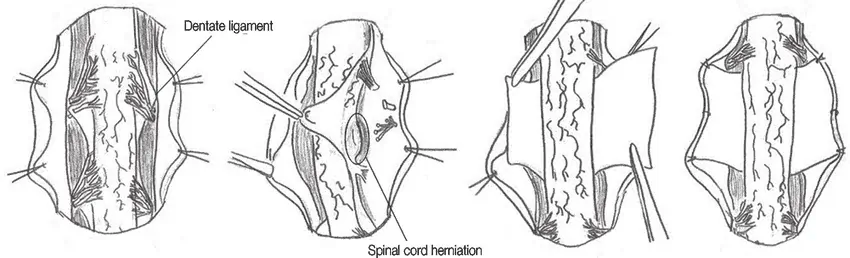
- Dynamic cord compression during neck flexion with forward displacement of the posterior dura is an unequivocal finding in the progressive stage However, this finding is absent in older patients who have reached a stable stage Some believe that a disproportional length between the vertebral column and the dural canal leads to a “tight” dural canal.
- The normal cervical dura is slack and consists of transverse folds during neck extension. With flexion, the length of the cervical canal increases In normal patients, the dural slack compensates for the increased length in flexion Patients with Hirayama dz may have an imbalance in the growth of vertebrae and dura, and the short dural canal cannot compensate; therefore, the dural canal becomes tight when the neck is flexed. Results in an anterior shift of the posterior dural wall, causing spinal cord compression
- The pathogenesis of cervical myelopathy may be ischemic changes or chronic trauma with repeated neck flexion. Compression may cause microcirculatory disturbances in anterior portion of the cord, leading to necrosis of anterior horns Changes are often greatest at C6 vertebral level Primarily affects the anterior horn cells, and in later stages of the disease, spinal cord atrophy ensues. Some autopsy studies report ischemic changes in the anterior horn cells, with asymmetric cord thinning.
- Flexion-extension images demonstrate forward migration of the posterior wall of dura Posterior epidural space enlarges with flexion and is seen as a crescent of high signal on T1 and T2 images Likely reflects congestion of posterior internal vertebral venous plexus Uniform enhancement of epidural space with contrast May have flow voids in epidural space Compressive flattening of the spinal cord with forward shifting of the posterior dura.
Symptoms of Hirayama Disease
- In terms of the signs and symptoms that are consistent for an individual who has monomelic amyotrophy are the following
- Muscle weakness
- Fasciculations
- Tremor
- Cold Hand
- Muscle cramps
The signs and symptoms of Hirayama’s disease can include:
- No pain
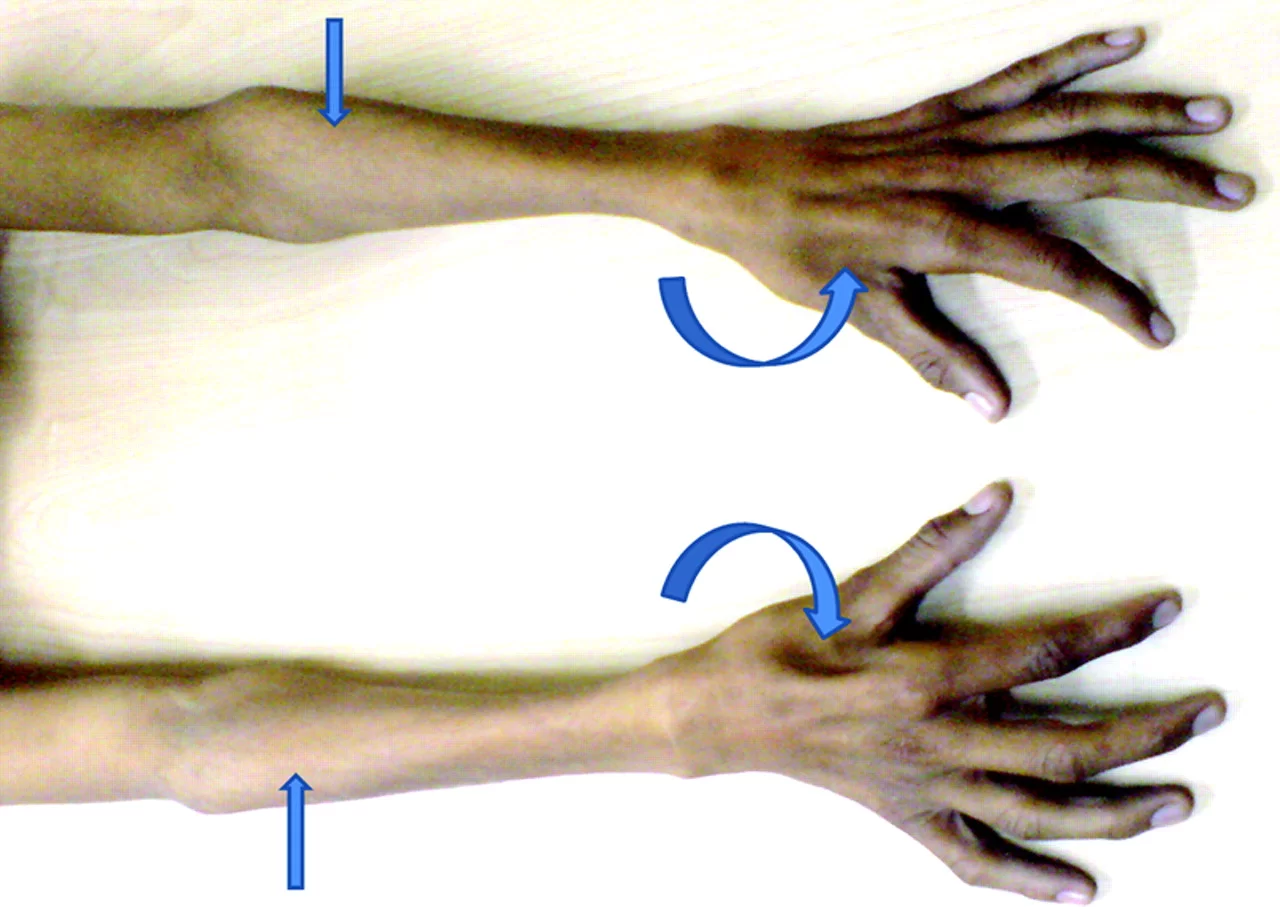
- Weak grip
- Clawed hand
- Hand tremors
- Weak hand muscles
- Wasted hand muscles
- Wasting of a single limb
- Weak lower arm muscles
- Weakness of a single limb
- Wasted lower arm muscles
- Fine motor control problem
Cause of Hirayama Disease
- The disability originates with impaired functioning of the anterior horn cells of the lower cervical cord (lower neck ) but the cause of the decline is not fully understood and is still considered unknown Hirayama believes that ” forward displacement of the cervical dural sac and compressive flattening of the lower cervical cord during neck flexion ” a loss of normal neck curvature (the cervical lordosis ) and cervical chord by the dural sac in forward flexion.
Differential Diagnosis
- Several conditions can be considered in the differential diagnosis of “Hirayama disease” including:
- amyotrophic lateral sclerosis, spinal muscle atrophy, C8-T1 radiculopathy, compressive myelopathy, cervical spondylotic myelopathy, syringomyelia, post-polio syndrome, multifocal motor neuropathy, and toxic neuropathy
- Myotonic dystrophy: An autosomal dominant genetic disorder, commonly seen in middle-aged men and traditionally identified with a tonic contraction of muscles in the upper limbs. It is associated with systemic changes including cataracts, pulmonary dysfunction, endocrine pathology, infertility, and cardiac conduction changes. It is distinguished from Hirayama by systemic involvement and EMG Findings, absent MRI findings, and muscle biopsy findings.
- Tephromalacie Anterieure: Anterior horn infarction demonstrated with muscle wasting of the distal upper limbs, caused by an occlusion of spinal arteries, commonly seen in middle-aged adults, and associated with arteriosclerosis. It presents bilaterally.
- Syringomyelia: Chronic central degeneration associated with motor and sensory changes seen in bilateral upper limbs, commonly seen after injury in geriatric populations without preference to gender. Structural changes can be seen on imaging.
- Pronator syndrome: Commonly presents unilaterally and is associated with a chronic injury. Symptoms increase with specific activities. Increased reports of pain help to identify this condition with physical findings and also indicate more than one peripheral nerve involvement.
Diagnosis of Hirayama Disease
( MR FINDINGS )
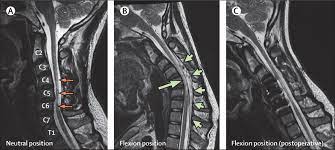
- Flexion-extension images demonstrate forward migration of the posterior wall of dura
- Posterior epidural space enlarges with flexion and is seen as a crescent of high signal on T1 and T2 images
- Likely reflects congestion of posterior internal vertebral venous plexus
- Uniform enhancement of epidural space with contrast
- May have flow voids in epidural space
- Compressive flattening of the spinal cord with forward shifting of the posterior dura.
- Spinal cord flattening is asymmetric in majority of cases. This is an important finding on routine nonflexion MR images and should raise suspicion.
- Spinal cord atrophy limited to the anterior horn cells found in later stages of the disease.
- Morphologic changes on MR images correlate well with clinical and electromyographic data
- Two flexion T1 post Gd images show increase thickening of posterior epidural space (arrows) which enhances and contains flow voids.
- Axial T1 post Gd images in same patient show thick epidural space, particularly posteriorly, compressing the spinal cord.
Electromyogram/Nerve Conduction Study
- EMG and NCS significant findings are noted in the C7, C8 and T1 innervated muscles. NCS have intermittently demonstrated decreased compound muscle action potential (CMAP) amplitude most noticeable in the median nerve.
- EMG findings are indicative of chronic denervation seen as a high amplitude of action potential with a prolonged duration, without active denervation (absence of positive sharp waves or fibrillation potentials) and no resting fasciculations in the C7, C8 and T1 innervated muscles. Findings are increased when the temperature is decreased.
Hirayama Disease of Physiotherapy Treatment
Conservative treatments
- Avoidance of neck flexion can stop the progression of the disease
- Some advocate application of a cervical collar for 3 to 4 years since the progressive stage usually ceases in a few years.
Strengthening Program:
- Electrical Stimulation to the muscles is supplied by the radial nerve, median nerve, ulnar nerve
- Exercise of the hand fingers on multi exercise


- putty exercise
- clay activities
- Gripping exercise
- Squeezing a sorbo ball
- picking and putting down objects
- Finger opening and closing
- Mild stretching
- Strengthening of all upper limb muscles with dumbles

Home Exercise Program
- Dough making
- unbuttoning of shirt
- Clay activities
- Squeezing exercise
Surgical options are there for this disease:
- Surgical intervention, including cervical decompression and/or fusion with or without duraplasty, may be an option.



One Comment