
Meniscus Tear
What is Meniscus Tear?
A meniscus tear is a common injury in the knee, specifically among athletes and sports persons. A meniscus tear can be induced by twisting, bending, and a direct blow to the knee. Signs of a meniscus tear contain swelling, pain while walking, and knee instability.
Meniscus tears can be painful and weakening. Sadly, it’s completely common. A meniscal tear is the most repeatedly happening cartilage injury of the knee.
Covers the bones from wear and tear. Though all it takes is a sufficient twist of the knee to tear the meniscus. In some patients, a part of the teared-up cartilage cracks loose and catches in the knee, pushing it to lock up.
Anatomy of Meniscus
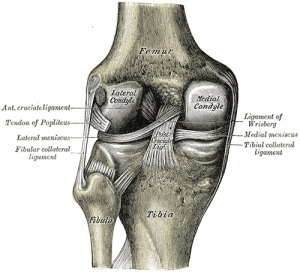
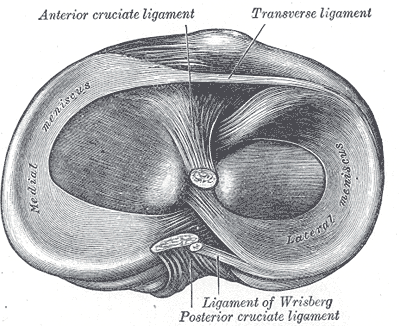
The knee joint mainly contains two menisci, which are constructed of fibrocartilaginous tissue and present between lateral condylar articulation and medial condyles of the tibia and femur. The knee meniscus directs to either the lateral or medial fibrocartilaginous structure. The menisci are also known as semi-lunar cartilages due to their curve shape.
Both menisci contain:
- Two ends, both connected to the tibia condyle
- Two borders – External border is wide, convex, and fixed to the fibrous capsule, and the internal border is narrow, concave, and free.
- Two surfaces – The upper surface is concave for presentation with the femur. The lower surface is matte and relaxes on the peripheral two-thirds of the tibial condyle. The peripheral wide part is an adequate blood supply. The internal part is avascular and sustained by synovial fluid.
The medial meniscus is almost semicircular, existing thicker behind than in front. The posterior fibers of the anterior end are constant with the transverse ligament of the knee joint. Its peripheral margin is sticky to the resonant part of the tibial collateral ligament.
The lateral meniscus is almost circular. The posterior end of the meniscus is connected to the femur via two meniscofemoral ligaments. The tendon of the popliteus muscle and the capsule separates this meniscus from the fibular collateral ligament in the knee joint.
Bio-mechanics of Meniscus
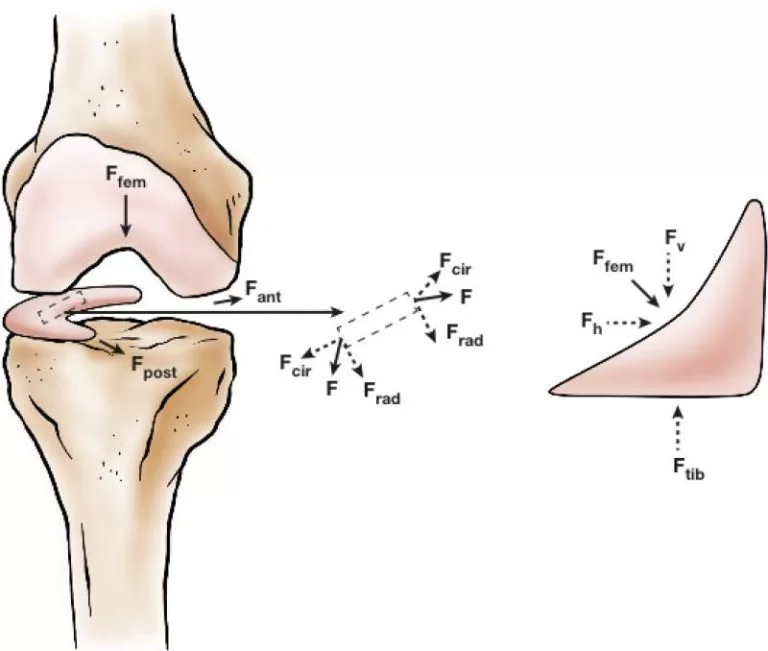
The menisci distribute the weight of the body and decrease conflict while activity. The condyles of the femur and tibia encounter at one point (which alters while flexion and extension of the knee). This varies from sesamoid bones, which are constructed of bony tissue and whose part mainly is to prevent the surrounding tendon and to improve their mechanical impact.
The meniscus resists many extra forces such as tension, shear, and compression. It even act an essential role in weight-bearing, weight transmission, shock absorption, as well as lubrication and nourishment for articular cartilage. These considerable and complex functions need a technical form. The tissue is wedge-shaped, which confirms positive adept at stabilizing the curved femoral condyle while presenting with the matte tibial plateau.
While daily activity, axial tibiofemoral powers squeeze the menisci. The wedge shape of the meniscus and its horn branches serve to transform the vertical compressive strengths into horizontal round pressures. At that exact time.
Symptoms of Meniscus Tear
You might feel a “pop-up” sound while a tear of the meniscus occurs. Most patients can even walk on their injured knees. Many athletes continue playing with their tears. After more than 2-3 days, your knee will slowly become more rigid and puffy.
- Knee Pain
- Knee joint immobility and bulge
- The sense of your knee “giving way”
- You aren’t capable to move your knee via its full range of motion
- A problem in flexing and straightening the leg
- A tendency for your knee to obtain “stuck” or locked
Causes of Meniscus Tear
- A meniscus tear can result from any movement that leads to strong twisting and rotating of your knee, such as forceful pivoting or impulsive stops and turns. Also kneeling, full squatting, or lifting something weighty can occasionally conduct in a meniscus tear. In aged adults(more than 40 years), degenerative changes of the knee may take part in a meniscus tear with no trauma.
- If you are sorrowing from knee osteoarthritis, you are at a higher chance of damaging your menisci. Knee osteoarthritis is a common joint illness in which pain and immobility in your joints are even induced by aging and wear & tear.
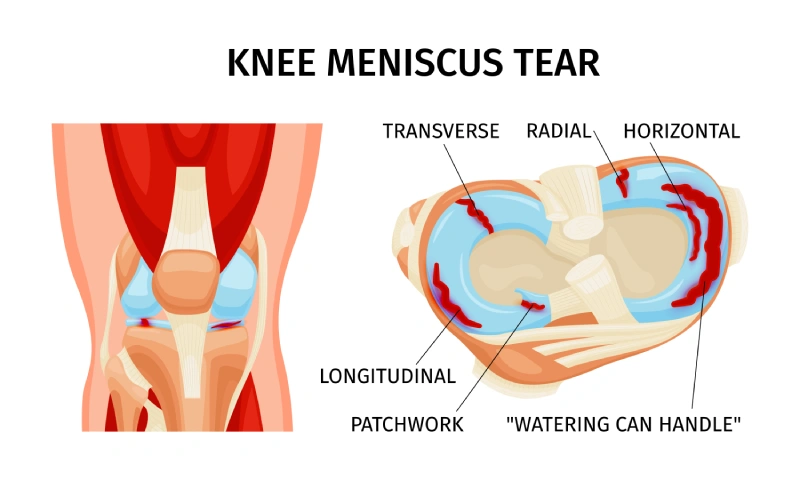
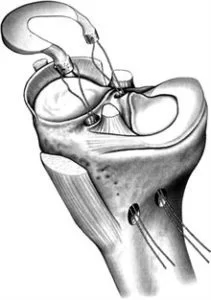
Types of Meniscus Tears
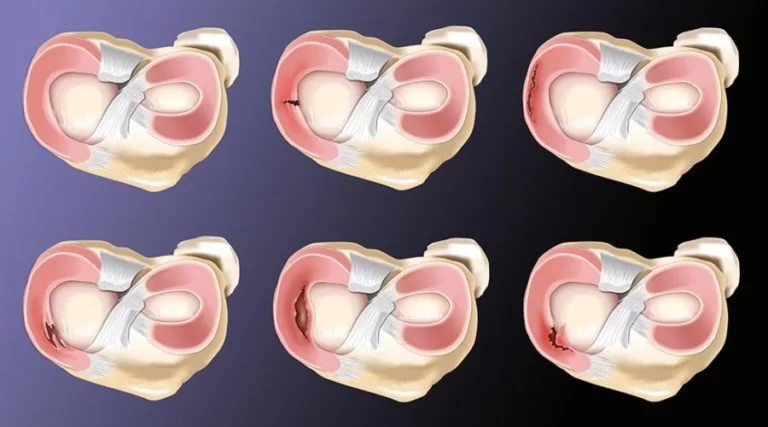
- Intrasubstance/Incomplete Tear: An incomplete tear is typically found on an MRI imaging test. As noticed in the upper left corner of the image, an incomplete tear commonly examines as normal at the moment of surgery. Usually, these are a symptom of prematurely degenerative modifications of the meniscus tissue, but rarely they are indications of a problem. Incomplete tears of the meniscus are steady damages, and they commonly don’t need any surgical treatment. By the period people are in their 20s/30s, intrasubstances tears of the meniscus tissue are very naturally seen on an MRI.
- Radial Tear: The radial meniscus tear shown in the center of the top row of the image, is the standard type of meniscus tear. These tears are within the avascular area of the menisci, where there is no adaptive blood supply, and hence there is little ability for these tears to recover. Consequently, when these tears come to need surgical treatment, naturally the only choice is to cut out the impaired portion of the menisci.
- Horizontal Tear: A horizontal tear is a tear that is commonly responsive to meniscus repair. As noticed in the upper right corner of the image, a horizontal tear goes along the peripheral fibers of the menisci. Preferably than extracting the impaired portion of the menisci, a horizontal tear can be capable to be along the peripheral fibers of the menisci. Instead of extracting the impaired part of the menisci, a horizontal tear may be capable to be stitched together. The key to choosing the treatment of these tears is their spot. If situated within the vascular part of the menisci(near the outer edge) then there is a recovery possibility, and thus repair. When situated more centrally, these tears won’t recover, even if corrected.
- Flap Tear: A flap tear of the meniscus, shown in the lowest left corner of the image, is a unique pattern of the tear. In occasions where the flap is inducing symptoms of detecting in the knee, generally, the flap of the meniscus may be extracted without extracting much tissue at all.
- Complex Tear: A complex tear means there is a mixture of tear patterns. Established in the middle image on the lowest row, a complex tear frequently affects both radial & horizontal tear patterns. Generally complex tears aren’t treated with meniscus repair due to the complicated nature of the tear. In some unique cases, some of the meniscus tears can be extracted, during other parts can be corrected.
- Bucket–Handle Tear: A bucket-handle tear is an extensive type of horizontal meniscus tear. These tears frequently lead to the knee becoming stuck inducing the tear portion of the meniscus to stop normal knee movement. Bucket-handle tears usually need more critical surgical treatment in demand to let the knee start flexing again.
Diagnosis of meniscus tear
- X-rays: Even though X-rays don’t suggest menisci tears, they can show different causes of knee pain, for example, osteoarthritis.
- Magnetic resonance imaging (MRI): MIR can produce adequate images of the soft tissues like ligaments, muscles, and cartilage of your knee joint.
- Arthroscopy: This method lets the doctor make a light incision into the knee joint into which he inserts a camera with a light connected to see straight inside the joint permitting it to see any impairment and to confirm the diagnosis and an instructed judgment on management possibilities.
Special test for a meniscus tear
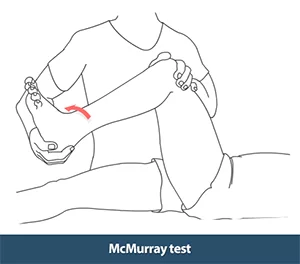
1. McMurray test:
The patient’s position is supine on the mattress with the hip and knee both bent. With the foot as near to the hip as possible, the therapist upholds the knee joint with fingers along the knee joint line with one hand, and the other hand spins the tibia medially and laterally during extending and bending the knee. If the test is positive indicating a meniscal tear, the patient will experience pain and the therapist will sense and/or hear meniscal motion when the meniscus is squeezed between the tibia and femur condyles.
2. Apley test (grinding) test:

The patient’s position is prone, with their knee bent to 90 degrees and their hip raised upward. The therapist involves axial force to the feet and turns the tibia medially and laterally. Pain and the ‘pop up’ sound present on compression indicates the test is positive.
Treatment of Meniscus tear
Treatments for meniscus tears are especially medical treatment, physiotherapy treatment, exercise, rest and the last choice is surgical treatment.
Medical treatment
Rest with some activity modifications.
Use an ice pack for your knee for 10 minutes, 2-3 times/day.
Compress your knee with a brace or knee cap to control more swelling.
Elevate your leg beyond your heart leave during icing it or whenever sleeping. Without treatment, a part of the meniscus may become lax and glide into the knee joint. This can lead to your knee slipping, popping, or locking.
Surgery for a meniscus tear
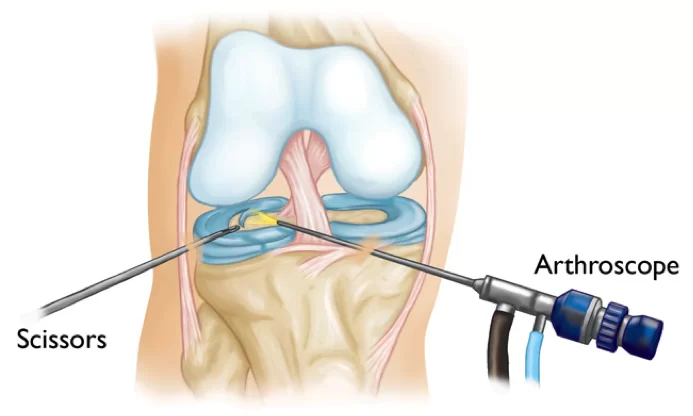
1. Arthroscopic Meniscectomy:
A meniscectomy is a process to extract the torn part of the meniscus. This method is distant more normally executed than a meniscus repair method. The meniscectomy is accomplished to clear the impaired part of the meniscus during leaving as much beneficial menisci as possible. The meniscectomy generally has a rapid rescue and permits for the quick resumption of movements using the knee joints.
2. Meniscus Repair:
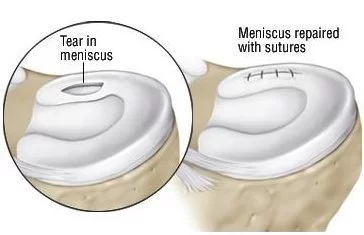
A meniscus repair is a surgical method done to repair the impaired menisci. The meniscus repair may reform the normal anatomy of the knee and has a better long-duration prognosis when successful. Regardless, meniscus repair is a better effective surgery, the recuperation is more prolonged, and due to the limited blood supply of the meniscus, it isn’t usually possible.
3. Meniscus Transplant:
Meniscus transplantation contains putting the meniscus from a dead donor patient into someone who has had their menisci removed.
The patient for a meniscus transplant is a person who had their menisci extracted and thereafter starts to produce knee pain.
A Meniscus transplant isn’t conducted for a critical meniscus tear, but instead when the subtraction of the whole meniscus has induced constant knee pain.
Physiotherapy treatment for a Meniscus tear
Not all meniscal tears need surgery, conservative treatment is another possibility. Physical therapy is one example of conservative treatment; it aims to strengthen the quadriceps muscle to control secondary quadriceps atrophy. This treatment is mainly successful in an incomplete meniscus tear or a small stable tear in the area with adequate blood supply. A menisci tear that indicates few, rare signs, will originally be treated conservatively.
Exercise therapy has been recommended to be a useful treatment choice for patients with knee degeneration(OA). Treatment aims to enhance knee function and reduce joint pain. There is substantial proof that physical therapy recreates an essential role in relieving symptoms and enhancing the muscle strength and physical ability of patients.
Acute Management
Physical therapy contains primarily RICE (Rest, Ice, Compression, Elevation) protocol when surgery is not essential.
RICE is very significant in the first 24 hours after an imperative soft tissue injury. Specifically when there are impaired blood vessels. It assists to decrease pain and swelling.
Cryotherapy, also known as ice application, is a process in which the body is contacted with a medium with a descending temperature. Using a cold source would reduce the temperature of the soft tissues. It induces external vasoconstriction and a reduction of local blood circulation. The common suggestion is to use ice for 10 minutes every 2 hours for the first 48-72 hours after onset.
- Meniscus tear brace:

A meniscus tear brace is created to supply assets and stability to the knee while movements may induce pain and discomfort. A meniscus tear brace consists of three components: an external shell, a center pad, and an internal strap. The shell supplies stability and limitations in movement. The center pad supplies cushioning and shelter for the knee. The internal strap provides extra reinforcement to the knee joint by connecting the external shell to the thigh. Meniscus tear braces are operated on to treat injuries such as an anterior cruciate ligament(ACL) tear.
A meniscus tear brace is an orthotic appliance that is operated to assist the knee while daily physical activity. Meniscus tears are typical injuries, specifically in sports for example basketball and soccer, where athletes are needed to make impulsive workouts during bearing weight on their knees. Meniscus tear braces nourish support for the knee and control the knee from hyperextending. They are clinically demonstrated to decrease pain and swelling while physical activity and can help to contain additional injury on the knee.
Physiotherapy treatment is pain relieving electrotherapy modalities such as Interferential Therapy(IFT), TENS, Ultrasound Therapy, and Exercise Therapy.
Strengthening and stretching exercises for the quadriceps and hamstrings muscles are necessary.
The method of increasing muscle power relies on the timing of the rehabilitation protocol but even on the patient’s reaction, the availability of tools, and the rehabilitation therapist’s preference.
Exercise Therapy
1. Static Quadriceps Exercise (SQE):
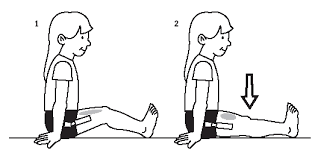
- Start by lying on your back with your lower limb straight.
- Put a little rolled-up towel beneath your knee.
- Push your knee down into the towel during pulling your quad muscle(front of thigh portion).
- Maintain it for 5 seconds, and then gradually remove the pressure over a towel.
- Do repeat 10 times.
2. Heel slide:
Executing heel slides is an excellent manner to enhance your knee flexion, or its capacity to flex totally.
To accomplish the heel slide activity:
- Start with lying on your back.
- Gradually slide your heel toward your buttocks, letting your knee flex as far as possible.
- Gradually let your heel slide and return to the straight knee position.
- Do repeat the movement 10 times, pushing gradually as you flex and straighten your knee.

3. Straight Leg Raise (SLR):

Straight leg raises are a good method to enhance hip muscle’s power to support your knees.
- Start with lying on your back with your affected knee straight outward and your other knee flexed.
- Constrict your quad muscle(thigh) on your straight leg and lift the leg to the flexed leg at knee level. Be sure to maintain your knee straight during the movement.
- Maintain your straight leg up for 5 seconds. Then drop it down gradually.
- Do repeat this exercise 10-15 times.
- You can execute straight leg raises in various positions. If you are lying on your side during accomplishing it, your gluteus medius muscles will be functioning. Your gluteus maximus will be functioning if you do the prone straight leg raise.
4. Prone hip extensor:
- Start with lying in a prone position, and raise your leg straight upward after you (toward the roof).
- Raise your feet approximately 6 in. (15 cm) off the bed, maintain for 5 seconds, then lower it down gradually.

5. Prone hang exercise:
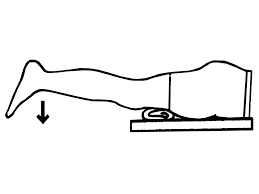
To enhance knee extension (straightening) range of motion, you can execute the prone hang exercise:
- Start with lying in a prone position with your foot beyond the edge of the bed.
- Let gravity force gradually drag down your knee into complete extension.
- Maintain this position for 15-30 seconds, then flex your knee.
- Do repeat 3-5 times.
6. Heel raise:
- Start in a standing position with your foot a few inches apart from each other, with your hands slightly relaxing on a chair in front of you.
- Gradually lift your heels off the base during maintaining your knees straight. Maintain for about 5 seconds, then gradually lower your heels to the ground.

7. Standing calf stretch:
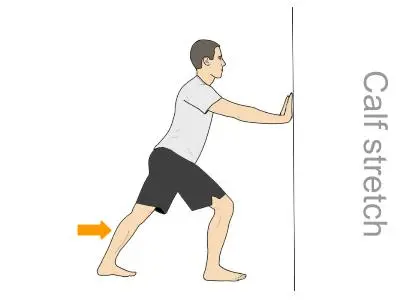
- Start in a standing position facing a wall with your hands on the wall at almost eye level. Hold your affected leg back with your heel on the ground. Maintain the other leg ahead with the knee flex. Rotate your back feet just inward (as if you were pigeon-toed). Gradually lean forward into the wall until you sense a stretch in the back of your calf. Maintain the stretch for 15-30 seconds. Then return to the starting position. Do repeat 3 times. Repeat this exercise 2-3 times/day.
8. Hamstrings stretch on the wall:
- Starting with lying on your back with your buttocks near a door. Stretch your normal leg straight out in front of you on the ground via the door. Lift your affected leg and rest it over the wall next to the door frame. Maintain your leg as straight as possible. You should experience a stretch in the back of your thigh. Maintain this position for 15-30 seconds. Do repeat 3 times.

Chronic Management
9. Step Up:

- Begin in a standing position with the feet of your involved leg on a support 3-5 inches high block like a small stair step up. Maintain your other feet flat on the ground. Move your weight into the affected leg on the support. Straighten your affected leg as the other leg comes off the ground. Then return to the starting position by flexing your affected leg and gradually lowering your normal leg back to the ground. Do 2 sets of 15 of this exercise.
10. Modified mini squats:
To accomplish mini squats in a modified position:
- Start standing with your legs apart from each other at shoulder-width.
- Flex your knees to around a 45-degree angle.
- Maintain this mini-squat position for 3-5 seconds.
- Gradually stand back up straight.
- Do repeat 10 times.

Joint Mobilizations
Decreased joint flexibility could be the impact of injury, edema, immobilization, and surgery. If immobilization develops it can lead to pain in the knee and also involve ankle mobility.
Joint mobilization is necessary for the following joints:
- Superior Tibiofibular joint;
- Patellofemoral joint. Patellar mobility is essential for a full flexion-extension of the knee;
- Tibiofemoral joint. It’s the most usually mobilized joint to enhance the range of motion in the knee movement.
Balance and Proprioception
Proprioception is the ability of your body to apprehend where it is in space. This is possible due to your joints and muscles articulating with your brainstem.
Occasionally after a meniscus injury, your proprioception evolves damaged. This may happen because of a period of immobilization after your injury.
Functioning with your physiotherapist on balance and proprioception exercises can be an essential part of your recovery program.
Some balance exercises to do may contain:
1. One-leg stance (do this with your eyes opened or closed)
2. Working with a BAPS board

3. Standing on a BOSU Ball

Balance and proprioception exercises should be difficult, but you should always stay safe during functioning them. Be sure you have a safe environment to exercise in and something to grab into.
Plyometrics and neuromuscular training
After 4-5 weeks of performing on correcting a normal ROM, strength, and balance, of the knee it can be time to begin to regain your capacity to run, jump, and land appropriately. This may help to replace high-level work and athletic movements.
Plyometrics is a type of exercise that includes learning to jump and land appropriately. This can help you revive optimal neuromuscular recruitment of the muscles near your hips and knees.
Working on plyometrics as a region of your meniscus recovery can help minimize tension and pressure near your knee while running, jumping, and executing cutting maneuvers during sports.
Plyometric exercises and neuromuscular activity for your knees contain:
- Single leg hopping
- Jump lunges
- Lateral plyometric hops
Bicycling
Riding a stationary bicycle can be an essential part of your meniscus tear exercise protocol. Bike riding may have multiple advantages, including:
- Enhancing the ROM of your knee
- Enhancing muscular endurance in your lower limbs
- Restricting tension and strain on your knee (compared with high-impact exercises for example running)
- Your physical therapist can help decide the portion of the time you should ride and the right quantity of resistance. In general, it is instructed you ride for 20-30 minutes, several days each week.
Conclusion
A meniscus tear can be a painful injury that can control you from appreciating your normal work and daily movements.
By functioning with your therapist and engaging in an active physiotherapy exercise program, you can fast and safely return to your maximal level of movement and function.
FAQ
Can a meniscus tear heal on its own?
In meniscus tears condition, people believe the injury will recover over time on its own. But the fact is that various types of meniscus tears will not heal without proper treatment. If the tear is on the outer one-third of the meniscus, it can recover on its own or be corrected surgically.
Which are 3 signs of a meniscus tear in the knee?
The standard symptom of a meniscus tear is included:
Pain.
Stiffness and swelling.
Catching or locking of your knee.
The sensation of your knee giving way.
Inability to push your knee via its full ROM.l ROM.
Which is the best treatment for a meniscus tear?
Your doctor may instruct the RICE protocol regimen of rest, ice, compression, and elevation to treat a meniscus tear. Relaxing your knee may help reduce your symptoms. Your physician can recommend using a cane for a few weeks to maintain the weight off your knee and to remain out from physical activity which can have contributed to the injury.
How long can a meniscus take to cure?
Generally, mild meniscus tears heal within 2-3 weeks. Signs of moderate meniscus tears: Pain at the side or center of the knee joint. Stiffness around the knee.
Are all meniscus tears repairable?
Since the meniscus helps to cover the knee from wear and tear, doctors attempt to repair the meniscus whenever possible. Regardless, most meniscus tears are not supposed curable. The meniscus has less blood supply, and tears in areas with little or no blood supply have a high chance of not recovering it’s own.





22 Comments