
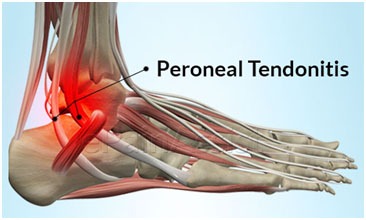
Peroneal tendinitis and physiotherapy treatment
- Peroneal tendinitis is a condition that can be acute or become chronic (peroneal tendinopathy) whereby there is an irritation to one or both peroneal tendons with subsequent degeneration and inflammation.
Anatomy related to peroneal tendinitis
- The peroneus longus and peroneus brevis muscles reside in the lateral compartment of the lower leg and are innervated by the superficial peroneal nerve.
- The peroneal tendons receive their blood supply from the peroneal artery and the tibialis anterior artery. There are 3 avascular zones that may contribute to tendonitis: in both the tendons at the turn around the lateral malleolus and in the peroneus longus tendon where the tendon curves around the cuboid.

- The peroneus longus arises from the head and proximal two-thirds of the lateral surface of the body of the fibula and the origin of the peroneus brevis is located on the distal two-thirds of the lateral surface of the body of the fibula, medial to the Peroneus longus.
- Both muscles become tendons proximal to the ankle joint and pass posterior to the lateral malleolus in a fibro-osseous tunnel, the retro malleolar groove.
- This groove is formed by the superior peroneal retinaculum (SPR), the fibula, the posterior talofibular ligament, the calcaneofibular ligament, and the posterior-inferior tibiofibular ligament.
- Both peroneal tendons are in a common synovial sheath behind the lateral malleolus, where they are held in place by the superior peroneal retinaculum to prevent subluxation of the ankle.
- Distal to the fibula, the tendons travel within individual sheaths, separated by the peroneal trochlea on the lateral surface of the calcaneus.
- The peroneus longus tendon turns medially between the cuboid groove and the long plantar ligament and inserts onto the plantar surface of the base of the first metatarsal and the lateral aspect of the medial cuneiforms.
- The peroneus brevis tendon continues directly to its insertion onto the tuberosity (base) of the fifth metatarsal.
- Therefore the peroneus longus tendon remains posterior and inferior to the peroneus brevis until the lateral aspect of the foot.
- The actions of the peroneus longus and brevis are plantarflexion and eversion of the foot in open kinetic chain motion.
- During weight-bearing, the peroneus longus acts as a stabilizer of the transverse arch of the foot, as well as a stabilizer of the first ray during propulsion.
Etiology of
Peroneal tendinitis
- Peroneal tendonitis is common in running athletes (particularly endurance running due to a high number of cyclic muscle contractions), young dancers, ice skaters, and sports requiring a frequent change of direction or jumping such as basketball, skiing and even horse riding lesion may be due to partial tears, complete ruptures, subluxation, tenosynovitis, a fractured os peroneum, or damage to the peroneal retinacula.
- Chronic lateral ankle instability and excessive subtalar and ankle varus rotation may cause damage to the peroneal tendons and their associated structures.
- Contributional factors for the development of peroneal tendonitis are tight calf muscles, inappropriate training, poor foot biomechanics such as over-pronation of the foot or excess eversion of the foot, inappropriate footwear and muscle weakness of them. peroneus longus.
- Other causes include severe ankle sprains, repetitive or prolonged activity, direct trauma’s, chronic ankle instability, fractures of the ankle or calcaneus, and peroneal tubercle hypertrophy.
- Tendonitis, in general, occurs when an individual returns to activity without proper training or after a period of extended rest. Specifically for athletes, the type of footwear, training regimen, and training surface can contribute to the problem.
- For workers increased hours, changes in workstation or changes in the type of labor can contribute to symptoms.
Symptoms of
Peroneal tendinitis
- Aching pain on the outside of the ankle, especially with activity.
- Pain that decreases with rest.
- Swelling or tenderness behind the ankle bone on the outside of the ankle.
- Pain and weakness when actively moving the foot in an outward direction.
- Pain when pushing off the ball of the foot during walking or running.
- Pain when walking on a sloped terrain that turns the foot inward, and the ankle outward.
Diagnosis of
Peroneal tendinitis
- A thorough subjective and objective examination from a physiotherapist can be sufficient to diagnose peroneal tendonitis.
- Plain film radiographs do not reveal soft tissue abnormalities; however, they are useful for excluding arthritis, bone abnormalities such as pes cavus, or fractures.
- Diagnosis may be confirmed with an MRI scan or ultrasound investigation showing oedema. Ultrasonography may be used for detecting all types of peroneal lesions.
- In chronic cases, or in cases that may be difficult to differentiate from lateral ankle ligamentous injury, computed tomography or magnetic resonance imaging may be helpful.
- T2-weight MR images often show visible accumulation of fluid within the peroneal tendon sheath. The thickening of the synovial lining may be appreciated with high-definition images.
- Tenography may be especially helpful in the chronic setting with suspected stenosis within the tendon sheath.
Examination
A thorough history should be taken prior to the examination.
- Observation:
- Attention should be paid to the overall alignment of the leg and posture of the hindfoot.
- Patients with hindfoot varus may subject the peroneals to increased forces that predispose to injury, or the varus might result from peroneal weakness.
- Look for the presence of swelling over the posterolateral aspect of the ankle.
- Palpation:
- Feel for warmth and muscle guarding and tenderness along the course of the tendons. Passive hindfoot inversion, passive ankle plantarflexion, active-resisted hindfoot eversion, and active-resisted ankle dorsiflexion provokes pain posterior of the lateral malleolus.
- Range of motion:
- Examination frequently reveals the painful limitation of subtalar joint range of motion secondary to muscle splinting.
- Pain may also be demonstrated with passive plantarflexion and inversion, or active dorsiflexion and eversion of the foot.
- Muscle strength:
- Muscle testing evaluation shows decreased peroneal muscle strength.
- The peroneal muscles can be isolated from each other by the peroneus longus and brevis tests If the peroneus brevis tendon alone is affected, the pain is located posterior and distal to the lateral malleolus.
- Peroneus longus tendonitis presents with pain along the lateral calcaneal wall extending to the cuboid.
- Tests:
- A provocative test for peroneal pathology has been described. The patient’s relaxed foot is examined hanging in a relaxed position with the knee flexed 90°.
- Slight pressure is applied to the peroneal tendons posterior to the fibula. The patient then is asked to dorsiflex and evert the foot forcibly.
- Pain may be elicited, or subluxation of the tendons may be felt.
- Testing of lateral ankle ligaments: lateral ankle ligamentous stability should be checked with the anterior drawer and ankle tilt test.
- Medical Management
- The primary aim of treatment is to afford pain relief, restore mechanics, and return the patient to their desired level of active participation.
- Patients diagnosed with peroneal tendonitis can be treated with non-steroid anti-inflammatory medication (NSAID) and decrease the level of the activity in order to relieve pain.
- There is a lack of evidence for the use of corticosteroids. Also, the use of lateral heel wedges can help to manage mild cases peroneal tendinitis.
- If nonoperative treatment is ineffective or failed after 3 to 6 months, an open tenosynovectomy is recommended. Postoperatively:-Patients are made non-weightbearing during the first 2 weeks.
- Then they are placed in a short leg weight-bearing cast or boot. The range of motion exercises and strengthening activities (eccentric exercise) is started 2 to 4 weeks after surgery.
Physiotherapy management
- Treatment for peroneal tendonitis includes a program of stretching, strengthening, mobilisation and manipulation, proprioceptive and balancing exercises, icing, ankle bracing, or taping during contact sports If symptoms are severe, a cast or ROM boot immobilization is prescribed for 10 days.
- After symptoms resolve, the patient begins a progressive rehabilitation program along with a gradual increase to full activity.
- Use of proper footwear and orthotics. It also may be necessary to get fitted for a custom foot orthotic (corrective inserts for your shoes) to reduce stress on your tendons.
- Manual therapy: Your physical therapist may use hands-on techniques (manual therapy) to gently mobilize the joints in your foot, ankle, and lower leg.
- Soft-tissue mobilizations may be performed to loosen tightness, increase circulation, and relieve pain and swelling.

- Range-of-motion exercises: You will learn exercises to help the ankle, foot, and toes move properly.
- These exercises will help improve the way you walk or run.
- Stretching exercises will help ease any tightness in the calf muscles and the tissues at the bottom of the foot.

- Strengthening exercises: Walking or running on uneven surfaces (grass, sand, gravel, or trails) requires a lot of strength to avoid added stress on the ankle.
- Your physical therapist may teach you resistance exercises with bands, weights, or medicine balls.
- These exercises will strengthen your ankle, foot, and lower leg muscles. Your exercise program will be based on your specific condition, needs, and goals.

- Functional training: As your symptoms, strength, and motion improve, your physical therapist will help you return to your previous level of activity.
- You may learn sport-specific exercises to improve your movements. Your physical therapist also will design a personal home-exercise program for you to continue to perform after your physical therapy sessions have ended.
- Following your home program will help you maintain and continue to build your ankle and foot strength.
other related posts :





3 Comments