
Pusher Syndrome: Physiotherapy Treatment
What is Pusher Syndrome?
- It is a clinical disorder which is to following to the left or right brain damage in which the patients actively push away from to the nonparticipant side, leading to the loss of the postural balance.
- This mechanism is underlying the disorder
- Related anatomy is recently identified.
- Investigation of the patients is with to the severe pushing behavior is see to the perception of the body posture in relation to the gravity is to altered.
- Patients are experience to their body as oriented “upright” when the body is actually tilted of the side of the brain lesion.
- In contrast the patients with this syndrome see to the no disturbed processing of the visual & vestibular inputs determining to visual vertical.
- Clinically it is present to the 5% of the all patients of the post-stroke
- In approximately 10% of the patients with the stroke is referred for the neurological rehabilitation
- Patient is into severely impaired such as the many limitations [ gait, standing or transfers]
Mechanism of the Pusher Syndrome :
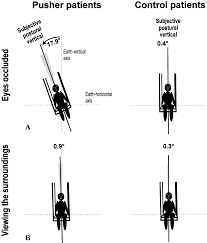
- Into this syndrome examined of to the ability of to the patients with the syndrome is to the determine of to the upright position while to the eyes are to occluded.
- The altered of to the perception of this body’s orientation is into the relation for to the gravity by using to a seating device which is allowed to the tilting of the patient for to the right or to the left without of to the ground contact.
- Patients are required to the indicate when to the reached of to the upright of body orientation.
- Mostly of the patients oriented to the upright posture is actually tilted of the 18 degrees of to the side of to the brain lesion .
- In the some patients show to no disturbed orientation in the perception of to the visual world [visual vertical]
- So that the in to the contrast of to the disturbed perception of to the upright body posture .
- Patients with to the this syndrome is in to the align of the longitudinal body axis of to the earth in the vertical upright when to the use the visual cues from to the laboratory ..
- Without to the a visual surround , become a complete darkness so that the patients are correctly determine to the visual vertical when to the sitting upright as well as to when the tilted in to the position .
- Results of the latter is to indicate of that to processing of to the visual & vestibular inputs for to the determination of the visual vertical is in unaffected by to the form the lesion.:
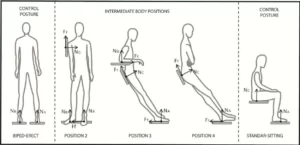
- In this syndrome three important variables are see in the patient .
- Spontaneous of the body posture is a tilt to longitudinal of to the torso toward of to the para tic side of to the body .
- Which is to a occurring onto a regular basis & not to only on to the occasion.
- It is a use in to the nonparticipant extremities which is to the create of to the pathological lateral tilt on to the body axis it is another sign to be noted to in this syndrome during to the diagnosis .
- In this condition includes to abduction & extension of to the extremities on to the non-affected side.
- It is to help in to the push toward the affected /paretic side.
- In this syndrome watch to the attempts of to the therapist for to the correct of this the syndrome which is posture by to the aiming to the realign of them into the upright posture which is resisted by the patient.
Causes of the Pusher Syndrome :
- An impaired of the somesthetic perception of the vertical
- Intact of the visual system
- Which is may be to consequence of the high-order of disruption of the somatosensory information processing from the paretic hemi-body.
- Affect the posterior thalamus
Symptoms of the Pusher Syndrome :

- Patients is problem to primary visual
- Visual perceptual problems impaired proprioception,
- Motor impairments,
- Relearn posture.
- Affected balance.
- Affected to gait
- Mostly problem in the standing and sitting
- Tilted of the body posture
Diagnosis of the Pusher Syndrome:
Spontaneous body posture:
- It is severe/moderate & mild
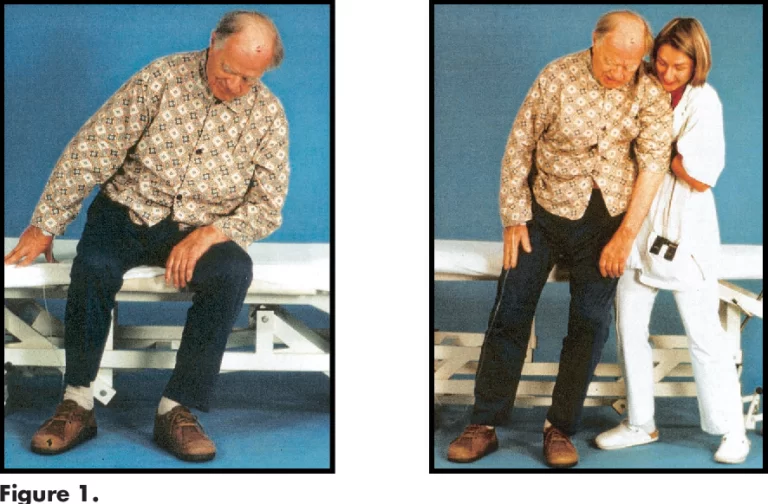
- The check & see The patient’s initial posture & then see the immediately after a positional change
- Like as to supine to sit or sit to stand.
- See the contra lateral tilting in this syndrome.
- Also see the postural abnormality regularly
Abduction and Extension of the Nonparetic Extremities:
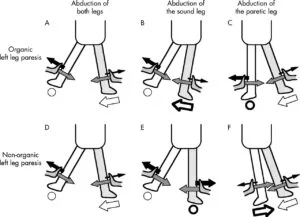
- Patients is demonstrate by the abnormal positioning of the side of the ipsilateral of to the brain lesion.
- Mostly to is abducted means away from the body.
- The elbow is held in to the extension.
- The hand is searching for to contact with a surface on which to the push to oneself for to upright position.
- In The lower limb is also abducted, with the knee & hip held in extension.
Resistance to Passive Correction of Tilted Posture:
- Patients is typically actively resist to against the therapist’s manual interventions to the correct their to body posture.Patient is to extended to upper & lower limbs for to used to the push to the weight towards to the paretic side.
- Subsequently, the SCP= Standardized Scale for Contraversive Pushing to be formulated on the 3 deficits.
- This scale is a useful tool for the clinicians to classify of this Syndrome
- It is a quick & easy to the apply in to the both an acute rehabilitation setting.
Scale for this syndrome:
Burke Lateropulsion Scale:
- This scale is assesses to the patient’s resistance to for .
- Passive to supine rolling.
- For to passive postural correction when to sitting & standing.
- To the assistance during form to the transferring & walking.
- Score of this each component s is rated onto a scale from to 0 to 3 & 0 to 4 to standing .
- The score is based on the severity of the resistance.
- The tilt to angle when the patient begins to resist the passive movement.
- The score for the diagnosis of this syndrome behavior is =2 points.
Scale for Controversial Pushing :
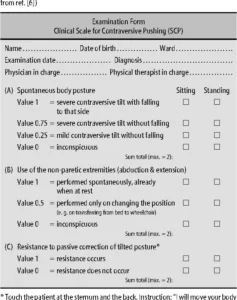
- It is made up of the 3 components.
- This symmetry of the spontaneous body posture to rated with the [0, 0.25, 0.75 & 1 point ].
- This use of the non-paretic to extremities [0, 0.5, or 1 point ].
- This resistance is to passive correction of this tilted posture [0 & 1 point ].
- For to a diagnosis of this Syndrome all to a 3 components need to be the present.
- The Burke Lateropulsion Scale is more sensitive to the Scale for the Contraversive Pushing.
Rehabilitation of the Pusher Syndrome:
- It is suggest of to the first goal is to the initial rehabilitation is to the provide of to the visual feedback of to the patient’s altered to the body posture.
- By providing the patients with the visual information in to a relation of their environment
- It is able to the feel into a erect posture when it see that it is tilted.
- Practicing to movements of the necessary to the reach a vertical body position.
- Performing to the functional activities while to a maintain a vertical body position.
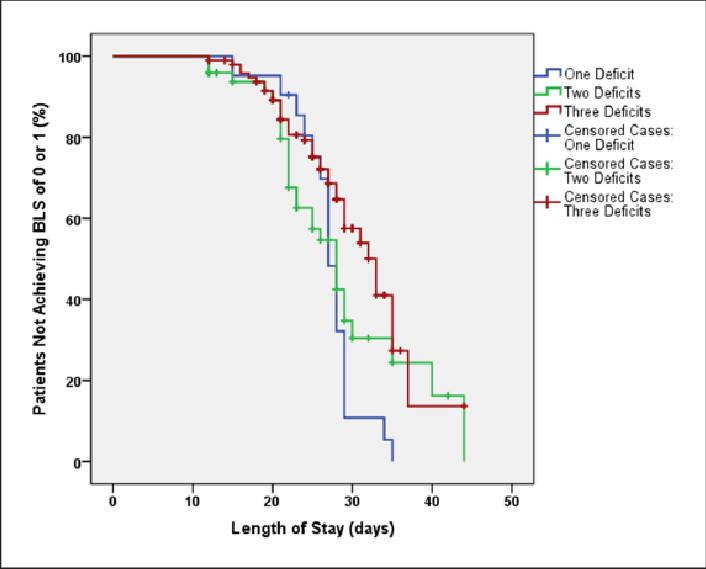
- It is suggested to that when the considering length of the rehabilitation stay to that laterality.
- Prognosis of this Syndrome which is considered to at the time of the goal setting for the rehabilitation.
Specialty Neurology of the Pusher Syndrome:

- This syndrome is a condition which is observed in to a some people which is following to a stroke which is left them to with the one side is weak due to the hemiparesis.
- Suffer of the exhibit to a tendency to the actively push away from to the unweak of to the side
- So that the leading to a loss of the postural balance.
- It is a result of the left or right brain damage.
- It is occurs in the contrast to the most stroke patients which is typically to prefer the more weight-bearing on to the non-hemiparetic side
- This abnormal condition is sever & leads to the loss of the postural balance.
- In the lesion is involved of this syndrome is to the though of the posterior thalamus on to the either side & the multiple areas of to the right cerebral hemisphere.
- This behavior is see to the perception of the body posture into a relation for to the gravity is altered.
- Patient is to the experience for the body as to the oriented to the upright posture when to the body is actually tilted the side of to the brain lesion.
- No disturbed processing of the visual & vestibular inputs
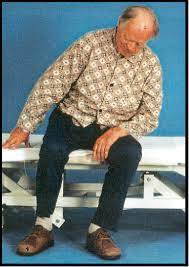
- In the sitting, the push is presents as a strong lateral lean toward the affected side
- In the standing it is creates to a highly unstable situation as to the patient is unable to the support to the body weight on to the weakened of the lower extremity.
- It is increased to risk of the falls addressed with the therapy for the correct to altered perception of the vertical.
- Patient feel the hemispatial neglect & aphasia
Physiotherapy treatment of the Pusher Syndrome :

- Physiotherapists is to focus onto the motor learning strategies in this patient.
- Verbal cues
- Practicing correct orientation
- Consistent feedback
- Weight shifting
- This all effective strategies are used to the for the reduce of the effects of this disorder .
- Patient is sit with the stronger side of to next to the wall & instructing to the patient for to lean towards to the wall
- It is a example of the treatment for this syndrome.
- New physiotherapy treatment for this patients are with syndrome is that to the visual control of to the vertical upright orientation which is to the undisturbed for in to all these patients
- It is the central element of the intervention in the treatment.
- Into the sequential of to the order, treatment is designed for the patients which is realize to their altered perception of the vertical
- Use visual aids for feedback about the body orientation
- Learn the movements which is necessary to reach for the proper vertical position & maintain the vertical body position while performing other activities.
FAQs
What is pusher syndrome after a stroke?
An unusual expression of abnormal body posture occurs in 5–10% of people with stroke. Pusher Syndrome is the name given to the activity of people who use their non-paretic limbs to push themselves toward their paretic side. It was first identified by Patricia Davis in 1985.
How common is pusher syndrome?
A person with pusher syndrome pulls away from their non-weak side after having a stroke. Fortunately, only approximately 5–10% of people who had a stroke develop this syndrome.
Where is pusher syndrome?
Damage to the posterolateral thalamus, a region of the brain, is most frequently linked to pusher syndrome. It has, however, also been noted in people who have had damage to the insula and postcentral gyrus. According to theories, these three brain areas are crucial in controlling upright posture.
What is pusher syndrome thalamic stroke?
Patients with “pusher syndrome” who have hemiparetic strokes express the odd behavior of deliberately pushing away from the nonparalyzed side with the unaffected arm or leg. This active opposing pushing results in a loss of postural balance if left unattended.




3 Comments