

Herniated Disc
Introduction
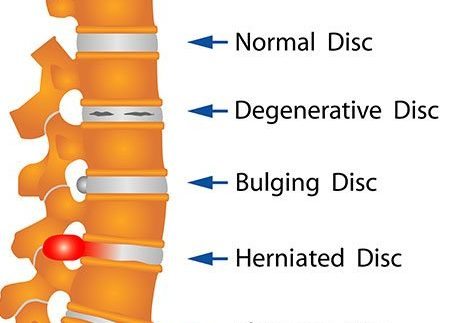
The vertebrae are a group of bones that are piled on top of one another to form your spinal column. The cervical spine has seven bones, the thoracic spine has twelve, and the lumbar spine has five. The sacrum and coccyx are near the base of the column. Discs provide cushioning for these bones.
By absorbing the shocks from routine motions like walking, lifting, and twisting, the discs shield the bones. Each disc is composed of a strong outer ring and a soft, gelatinous inside half. The interior part of the disc may poke through the outer ring due to damage or weakness. This condition is referred to as a prolapsed, herniated, or slipped disc.
Pain and discomfort result from this. You might also feel pain and numbness along the affected spinal nerve if the slipped disc compresses it. In extreme cases, surgery might be necessary to remove or correct the slipped disc.
Clinical Anatomy
Intervertebral discs: An intervertebral disc connects two neighboring vertebral bodies. They form the “Functional Spinal Unit (FSU)” along with the matching facet joints. The disc is made up of two cartilaginous endplates, a nucleus pulposus, and an annulus fibrosus. Only in youth is it possible to distinguish between annulus and nucleus because, as people age, the disc’s uniformity gets more consistent.
Therefore, after the age of 70, nuclear disc protrusions are uncommon. From a clinical perspective, it is crucial to regard the disc as a single, cohesive unit, the normal operation of which is heavily dependent on the integrity of each component. This implies that when one component is damaged, the others will react negatively. The disc contains an endplate, an annulus fibrosus, and a nucleus pulposus.
Causes of Herniated Disc
The tight collagenous ring that surrounds the nucleus pulposus is called the annulus fibrosus, and it makes up an intervertebral disc. When all or a portion of the nucleus pulposus pokes through the annulus fibrosus, disc herniation takes place.
- The most frequent cause of disc herniation is a degenerative process where the nucleus pulposus weakens and loses moisture as people get older. A progressive disc herniation that may result from this process may cause symptoms.
- Trauma is the second most common cause of disc herniation.
- Congenital conditions like short pedicles and connective tissue abnormalities are other reasons.
- The lumbar and cervical spines are the most frequently affected by disc herniation. Because of the biomechanical pressures in the flexible portion of the spine, disc herniation is more common in the cervical and lumbar regions. Disc herniation is less common in the thoracic spine.
- Herniated discs are thought to be caused by a combination of the bulging nucleus pulposus mechanically compressing the nerve and the localized rise in inflammatory chemokines. Because the annulus fibrosus is thinner and does not have the anterior or posterior longitudinal ligaments to support it structurally, a herniation is more likely to occur posterolaterally. A posterolateral herniation is more likely to compress the nerve root because of its close proximity.
- On the other hand, a significant midline disc herniation may result in spinal cord compression and clinical myelopathy. Herniated disc pressure on the longitudinal ligament and chemical irritation from local inflammation combine to cause localized back pain.
Signs and symptoms
One side of the body experiences the pain the most frequently. Depending on where the damage occurred, symptoms can vary and include the following:
- You may experience numbness in certain areas of your leg, hip, or buttocks and severe pain in others if you have a herniated disc in your lower back.
- Additionally, you can experience numbness or pain in the sole of your foot or the back of your calf. Additionally, the same leg could feel weak.
- You may have pain when moving your neck, a deep ache above or close to the shoulder blade, or pain that radiates to your fingers, forearm, and upper arm if you have a herniated disc in your neck.
- Additionally, you may get numbness in your fingers, forearm, elbow, and shoulder. Usually, the pain begins gradually.
Things might be worse:
- After sitting or standing
- At night
- While coughing, laughing, or sneezing
- When walking more than a few yards or meters, or bending backward
- When holding your breath or straining, like during a bowel movement
- You can also be weak in some muscles. You might not always be aware of it until you are examined by your healthcare physician. In other situations, you may find that you struggle to stand on one side of your body, lift your arm or leg, squeeze tightly with one hand, or have other issues. You can become unable to control your bowels or bladder.
- Some people may be asymptomatic.
- Slow and deliberate tip-toe walking.
- Antalgic or Trendelenburg gait.
Over the course of the week to months, the pain, numbness, or weakness frequently disappears or significantly improves.
Types of Herniations
- A posterolateral disc herniation is a protrusion into the spinal canal. The next lower nerve is typically compressed by a protruding disc as it passes over the disc on its way to the foramen. As an illustration, L5 protrusion typically impacts S1.
- Central (posterior) herniation is less common. A protruding disc above the second vertebra might cause Cauda Equina Syndrome or compress the spinal cord itself.
- Lateral disc herniation is a compression of the nerve roots that occurs above the herniation. The L4 nerve root is most frequently affected.
Stages of degenerative changes
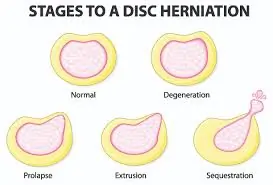
Stage 1: Initial Changes (Disc Degeneration)
- Dehydration of the disc: Dehydration results from the intervertebral discs’ diminished capacity to hold water in the early stages of DDD. The disc height decreases as a result, and the distance between neighboring vertebrae may also decrease.
- Minor Tears and Cracks: The annulus fibrosus, the disc’s outer layer, is susceptible to minor tears and cracks. These may increase the likelihood of future injury and disc instability.
- Mild pain and discomfort:
- At this point, people may feel mild to moderate back discomfort, particularly after engaging in physical activity or sitting for extended periods of time. Conservative therapy can be used to manage the discomfort, which is frequently irregular.
STAGE 2: Prolapse (bulging disc)
- Disc Bulging: As the illness worsens, the disc may protrude outward as the nucleus pulposus, the inner core of the disc, presses against the weakening annulus fibrosus. This may exert pressure on nearby structures, including the spinal cord and nerves.
- Greater discomfort and pain: People may feel more intense and ongoing discomfort, which frequently travels to their arms or legs. This is because the bulging disc is compressing the spinal cord or nerves.
STAGE 3: Herniation (ruptured disc)
- The disc Herniation: The outer disc layer may rip or rupture at this point, allowing the inner nucleus pulposus to protrude through the annulus fibrosus. A herniated disc, or slipped disc, is a popular name for this problem.
- As well as additional symptoms including numbness, tingling, and muscle weakness in the areas serviced by the damaged nerves, herniated discs can induce excruciating pain that is frequently persistent. Depending on the amount and location of the herniation, these symptoms may vary in intensity.
STAGE 4: Severe degeneration (advanced changes)
- Loss of Disc Height: The gap between the vertebrae may narrow as a result of the affected discs losing a considerable amount of height in the later stage of DDD.
- Osteophytes: The body may produce bony growths called bone spurs along the margins of the vertebrae to make up for the instability and loss of disc height. These may also affect spinal structures and nerves.
- Chronic and unbearable pain: At this point, people may have limitations in their everyday activities, decreased mobility, and persistent and exhausting pain. In order to stabilize and manage discomfort, surgery may be recommended.
Differential Diagnosis
It is important to consider that there are numerous pathologies that can mimic a herniated disc from both a clinical and imaging perspective.
Among these lesions are those that come from the
- Osteophytes and metastases in the vertebral body
- discal cyst in the intervertebral disc
- neuromas in the intervertebral foramina
- synovial cyst in the interapophyseal joints, hematoma, and epidural abscess in the epidural space.
Additional differential diagnoses consist of
- Spondylolysis
- Spondylolisthesis
- Cauda Equina Syndrome
- Muscle spasm
- Mechanical pain
- Myofascial pain (causes sensory abnormalities and local and/or transferred pain)
Among the spinal reasons are
- Osteomyelitis is an infection from trauma.
- Arachnoiditis and ankylosing spondylitis are examples of inflammation.
- Multiple myeloma, extradural tumors, and neoplasms—whether benign or malignant—that cause pressure on nerve roots.
Among the extraspinal reasons are
- Peripheral vascular disease
- OA hip
- Lesions in peripheral nerves
Complications
- Cauda Equina Syndrome
- Permanent nerve damage with persistent discomfort
- Lack of motion
Investigations
Physical Examination
Common signs of a single nerve lesion in the cervical spine caused by a herniated disc
- C5 Nerve: weakness during shoulder abduction, external rotation, elbow flexion, and forearm supination; pain in the neck, shoulder, and scapula; and numbness in the lateral arm. The brachioradialis and biceps are the muscles that are impacted.
- The C6 nerve causes discomfort in the neck, shoulder, scapula, and lateral arm, forearm, and hand. It also causes numbness in the thumb, index finger, and forearm. It is typical to experience weakness during external rotation, elbow flexion, shoulder abduction, and forearm pronation and supination. The brachioradialis and biceps are the muscles that are impacted.
- C7 Nerve: numbness in the palm, middle finger, and index finger, as well as pain in the neck, shoulder, and middle finger, are typical. In addition to weakness during radial extension, forearm pronation, and wrist flexion, elbow and wrist weakness are prevalent. The triceps is the muscle that is impacted.
- C8 Nerve: numbness in the medial hand and forearm, pain in the neck, shoulder, and medial forearm. In addition to distal thumb flexion, weakness is frequently observed during finger extension, wrist (ulnar) extension, distal finger flexion, extension, abduction, and adduction. Reflexes remain unaffected.
- T1 Nerve: numbness is common on the anterior arm and medial forearm, whereas pain is common in the neck, medial arm, and forearm. Thumb abduction, distal thumb flexion, and finger abduction and adduction can all result in weakness. Reflexes are unaffected.
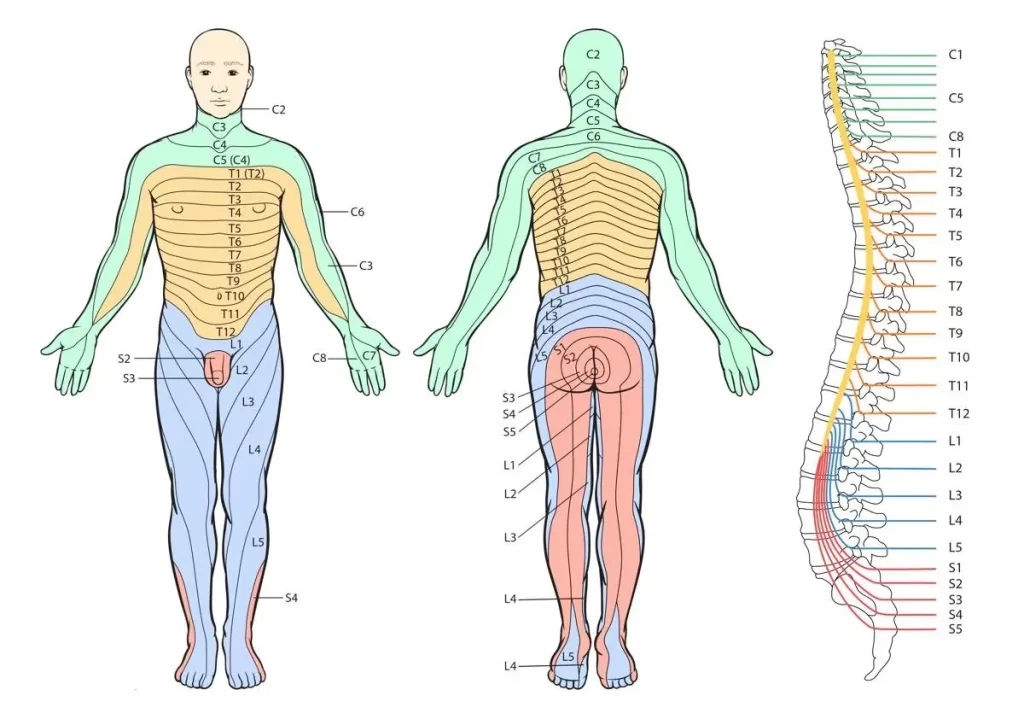
Common signs of a single nerve lesion in the lumbar spine include a herniated disc, compression:
- In the inguinal area, L1 nerve discomfort and sensory loss are prevalent. Neither the stretch reflex nor hip flexion weakness is impacted.
- Nerves L2-L3-L4: loss of sensation in the anterior thigh and occasionally the medial lower leg; weakness in hip flexion and adduction; weakness in knee extension; reduced patellar reflex; back discomfort that radiates into the anterior thigh and medial lower leg.
- L5 Nerve: back, extending into buttock, lateral thigh, lateral calf, dorsum of foot, and great toe; loss of sensation in the lateral calf, dorsum of the foot, and web space between first and second toe; weakness in hip abduction, knee flexion, foot dorsiflexion, toe extension and flexion, and foot inversion and eversion; reduced semitendinosus/semimembranosus reflex.”
- S1 Nerve: back, radiating into the buttock, lateral or posterior thigh, posterior calf, lateral or plantar foot; sensory loss on hip extension, knee flexion, and plantar flexion of the foot; Achilles tendon; medial buttock, perineal, and perianal region; weakness may be slight, accompanied by fecal and urine incontinence and sexual dysfunction.
- S2-S4 Nerves: absence of bulbocavernosus and anal wink reflexes; sensory deficiency on the medial buttock, perineal, and perianal areas; sacral or buttock pain spreading into the posterior portion of the leg or the perineum.
Special Tests
Cervical
- Upper limb tension test.
- Distraction test.
- Shoulder abduction test.
- Spurling test.
- Tinel’s sign
Lumbar
- The straight leg raise test: During this portion of the examination, the patient rests on his or her back while the physician helps raise the leg that is causing pain without bending it. This movement may indicate irritation or compression of a sciatic nerve root if it causes or increases discomfort in the lifted leg. When identifying a lumbar disc herniation in any of the two lower levels of the lumbar spine—the L4-L5 spinal segment or the L5-S1 spinal segment—this test is especially helpful.
- The contralateral (crossed) straight leg raise test: This test, which is a variant of the straight leg raise test, entails lifting the leg that is symptom-free. A sciatic nerve root may be irritated or compressed if lifting this leg causes discomfort in the opposite (non-raised) leg. The Fajersztajn sign, or the “well-leg” rise test, is another name for this exam.
- Lasègue’s Test: same as the straight leg raise test
- Bowstring test: Maintain this leg posture while flexing the patient’s knee to a 20° angle. The symptoms should subside as a result. After a positive test, applying pressure to the popliteal region will cause symptoms and create increased pain.
- Prone knee bending: The patient’s knee is passively flexed to end range by the examiner, who holds it there for forty-five seconds. Rotating the hip is not advised. Anterior thigh pain could be a sign of neural stress in the femoral nerve or a tight or strained quadriceps muscle. Lumbar radiculopathy of the L2-L3 nerve roots may manifest as pain in the posterior thigh, buttock, or unilateral lumbar region.
- Muscle Weakness or Paresis
- Reflexes: A reflex hammer is used to tap a tendon on the leg and/or foot in order to test the affected limb’s tendon reflexes. The doctor can identify the precise nerve root involvement and the extent of a potential herniation by looking for a lack of reflex reaction.
- Hyperextension Test: While keeping the knees extended, the patient must passively move the trunk through its whole range of extension. If the radiating pain worsens, the test shows that a disc herniation is the cause.
- Manual Testing and Sensory Testing Look for hypoaesthesia, hypoalgesia, tingling, or numbness.
Imaging tests
X-rays
The majority of clinics and outpatient offices have easy access to X-rays. Any structural instability can be evaluated using this imaging method. If X-rays reveal an acute fracture, an MRI or CT scan must be performed to thoroughly examine the condition.
Magnetic Resonance Imaging (MRI)
Imaging investigations using magnetic resonance imaging (MRI) are essential for seeing the spinal cord or spinal nerves and spotting anomalies. Images from an MRI can be used to pinpoint the location of the herniated disc and identify the nerves that are impacted. Additionally, an MRI can be used to rule out discomfort that is not connected to the spine.
Computed Tomography (CT) scan
A computed tomography (CT) scan creates images of your spine and the structures around it by combining many X-rays taken from various angles. Disc herniation cannot be seen on an X-ray; hence, CT scans aren’t used as frequently for diagnosis.
Electrodiagnostic tests
These tests are less common, but your doctor might use them to check for compression or damage to any of the nerves in your spine. A tiny needle electrode is placed into the muscle during electromyography (EMG) to record the electrical activity of your muscles both during rest and contraction. The ability of a nerve to transmit impulses to the muscles or along the nerve is assessed by a Nerve Conduction Study (NCS).
Outcome Measures
Other outcome measures can be employed if the disc herniation is symptomatic:
- Short Form-36 bodily pain (SF-36 BP)
- Oswestry disability index
- Roland-Morris disability index
- VAS score: one of leg pain and one of back pain
- McGill Pain Questionnaire: This questionnaire looks at the location, intensity, quality, and pattern of the pain as well as alleviating and aggravating factors.
Risk factors
Your risk of a herniated disc may be elevated by specific variables. They consist of:
- Gender: The majority of men with herniated discs are between the ages of 20 and 50.
- Inappropriate lifting: A herniated disc may result from lifting heavy objects with your back muscles rather than your legs. Your back may become vulnerable if you twist while lifting. Your spine might be protected if you lift with your legs rather than your back.
- Weight: Being overweight puts additional strain on your lower back’s discs.
- Repetitive tasks that cause back pain. Many jobs need a lot of physical labor. Some things need to be lifted, pulled, bent, or twisted all the time. You may protect your back by using safe lifting and movement techniques.
- Regular driving: Your spine and discs may experience strain from prolonged sitting as well as vibration from the car’s engine.
- A lifestyle that is neither active nor sedentary. A herniated disc is among the many medical disorders that can be avoided with regular activity.
- Smoking is believed to accelerate degeneration by lowering the oxygen flow to the disc.
Treatment
Medical Treatment
The majority of acute cervical and lumbar radiculopathies caused by herniated discs are treated non-surgically.
- The first-line treatment options are physical therapy and NSAIDs.
- Oral steroids, such as methylprednisone and prednisone.
- Low-dose benzodiazepines.
- The second-line methods are selective nerve root blocks and translaminar epidural injections. These are effective ways to deal with incapacitating pain.
- Patients with neurological impairments or those who don’t respond to conservative treatment require prompt surgical consultation.
Surgical Treatment
Who needs surgery?
- Surgery is not usually necessary for herniated discs. The symptoms will go away in a few days to weeks for about 90% of people.
- On occasion, though, a spinal column nerve may be compressed by the herniated disc. The area of the body where the nerve travels may become painful, numb, or weak as a result.
- The degree of discomfort and disability may influence the doctor’s recommendation for surgery.
- Rarely, the nerves that regulate the bladder and bowel may be impacted by a herniated disc. In order to restore bladder and bowel function and relieve pressure on the nerves, surgery will be required.
- A person might wish to seek treatment in a hospital that makes surgical decisions using a multidisciplinary approach, if at all possible.
Procedures:
- Open discectomy: To remove the herniated portion of the disc, the surgeon does open surgery.
- Endoscopic spine surgery: The surgeon uses an endoscope, a long, thin tube, to remove the herniated disc section.
- Surgery on the spinal disc core: The surgeon accesses the spinal disc core with instruments and then removes it with a vacuum. The spinal disc contracts as a result, releasing pressure on the nerve. Surgery is only possible if the outer layer of the disc is intact.
- Laminotomy or laminectomy: The portion of the vertebrae that covers and shields the spinal canal is called the lamina. In order to repair a herniated disc, surgeons may occasionally need to remove all or part of the lamina. A laminectomy removes the entire lamina, whereas a laminotomy removes only a portion of it. In both treatments, a small incision is made over the herniated disc in the middle of the neck or back. The surgeon removes the herniated disc by performing a discectomy after removing all or part of the lamina.
- Spinal fusion: To stabilize the spine after a laminotomy or laminectomy, a spinal fusion (SF) can be required. In an SF, screws are used to connect two bones. After undergoing an SF, some people may feel pain and that their motions are being restricted. The location of the herniated disc determines the likelihood of requiring an SF. Lumbar laminotomies usually call for an SF.
- If the surgeon does a cervical laminotomy from the front of the neck, an SF is necessary. If the surgeon does the same treatment from the back of the neck, an SF is rarely used. The precise position of the herniated disc determines the point from which the physician operates. Instead of an SF, some laminotomy patients may be candidates for artificial disc surgery.
- Artificial disc surgery: An alternative to spinal fusion is artificial disc surgery (ADS). In ADS, the surgeon inserts an artificial disc in lieu of the injured one.
Risk factors:
- Bleeding infections.
- Damage to the protective coating of the spine
- Damage to the nerve
Physical Therapy Treatment
Recovery from herniated discs frequently relies heavily on physical therapy. Including the following important points
- Ambulation and exercise resumed
- Pain Management
- Instructions on how to maintain a healthy weight
Programs for physical therapy are frequently suggested for the management of pain and the recovery of neurological and functional impairments linked to symptomatic disc herniation.
Patient Education
The patient is advised to avoid the activities that aggravate the symptoms, like forward bending and prolonged sitting, which can increase the pressure on the disc and thus aggravate the condition. Lifting heavy objects and sudden twisting and turning movements that put stress on the back should also be avoided.
Active exercise therapy
Symptomatic disc herniation can be treated with a variety of exercise regimens.
- aerobic exercise (such as cycling or walking) and preferred direction (McKenzie approach)
- flexibility activities, such as stretching and yoga
- exercises to improve proprioception, balance, and coordination (medicine ball and wobble/tilt board), as well as strength.
- Exercises for motor control MCEs.
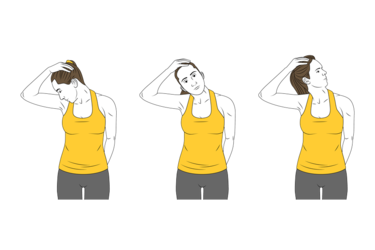
Exercises for cervical herniated disc
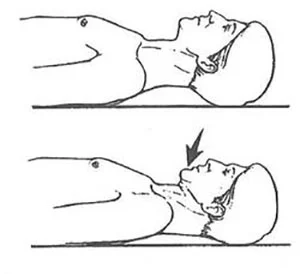
- Extension of the neck
- Place the base of your neck against the edge of a table or bed while lying on your back.
- Lower your head backward and let it hang there slowly and gently. Don’t proceed if this increases your pain or causes pain to radiate down your arm.
- Repeat five to fifteen times while holding this position for one minute and taking a one-minute break.
- Head lift combined with neck extension
- With your head dangling over the structure and your arms by your sides, lie on your stomach on a table or bed.
- Extend your neck against gravity and slowly and gently elevate your head.
- Neck retraction (chin tuck)
- Place your hands by your sides and rest your head on the bed while lying on your back.
- To create a double chin, tuck your chin in toward your chest.
- For five to ten seconds, hold this position. Repeat 15–20 times.
- Shoulder retraction
- With your arms at your sides, take a seat or stand against a wall.
- Put your elbows in a 90-degree bend.
- With your shoulders lowered and back, squeeze your shoulder blades together and drive the rear of your arms toward the wall.
- An isometric grip
- Remain upright and let your shoulders drop. Press a hand to your forehead.
- Keep your head in place and press it into your hand.
- For five to fifteen seconds, hold this position. 15 times over, repeat.
Stretches for cervical herniated disc
- Lateral bend
- Remain upright and let your shoulders drop.
- As though touching your ear to your shoulder were possible, slowly turn your head to one side.
- After 30 seconds, maintain this posture and take a break. Throughout the day, repeat three to five times.
- Scalene stretch
- Remain upright and let your shoulders drop.
- Put your left hand on the chair you’re sitting in and lower your shoulder blade.
- Gently bend your right ear back a little and down toward your right shoulder.
- Maintain this posture for 30 seconds, take a break, and then do it three to five times during the day.
- Rotation of the neck
- Relax your shoulders and sit up straight.
- Turn your head to the side gently. Don’t twist your neck or turn your head too far behind you.
- Turn your head to the opposite side slowly.
- Each position should be held for 30 seconds. Do this three to five times during the day.
Exercises for a lumbar herniated disc
Decompression of the Spine
How it works: The greatest exercise to begin with, if you have back pain linked to a herniated disc, is spinal decompression. It lowers the pressure that might be causing you pain and provides much-needed space between your vertebrae.
How to do it: To complete this workout, locate a spot where you can hang off a bar. For three rounds, the objective is to attempt to hang from the bar for 30 seconds at a time. Continue with additional workouts after a gradual release.
Half-Cobra Pose (Lumbar Extension Prone)
How it works: To promote better healing, the Half Cobra Stretch helps to press the disc material back towards the intervertebral disc’s center. Repetitive lower back extension is intended to achieve “centralization of symptoms,” which essentially implies that discomfort that radiates down the affected leg and foot should return closer to the low back, hence reducing the pain.
How to do it: Start by resting on your stomach in the prone position. Then, carefully raise yourself up on your elbows while maintaining a flat hip position.
-Return to the prone position, which entails lying face down, after holding the prop-up posture for ten to fifteen seconds. Increase gradually until you can hold the final position for 30 seconds. Try to complete this stretch ten times.
-You may not be able to manage this position at first, so start out slowly and carefully. If you feel any pain during your workout, choose a different one.
Full Cobra Pose (Advanced Extension)
How it works: This stretch is based on the same principle as the half-cobra posture mentioned before. This improved extension helps drive disc material back toward the middle of the intervertebral disc, which lessens pain perceptions.
How to do it: The more challenging variation of this stretch can be performed after you have perfected the half-cobra stance. Slowly raise your hands from the prone posture (stomach facing down) while maintaining a relaxed lower back and a floor-contact pelvis.
– Hold the prop-up position for 10 seconds. Do this stretch as many as ten times. Try maintaining this position for 20 to 30 seconds at a time if it is comfortable.

Standing Extension
How it works: This standing extension aids in reversing your usual habit of hunching. This stretch aids in returning the disc to its neutral position because the majority of bulging discs and herniated discs are caused by bad posture and repetitive flexion of the spine, particularly bending forward.
How to do it: To start this workout, stand up straight and keep your posture correct. Let both hands rest on your lower back now. Now use your hands to press your pelvis forward and lengthen your spine back. Continue to extend your neck until your back touches the ceiling. Work your way up to two or three sets, starting with ten repetitions. Start with ten repetitions and work your way up to three or four sets. This is an amazing exercise to perform when you need a break from sitting at your desk.
** This shouldn’t cause any pain. It’s not a good one for you if it makes you uncomfortable. If so, stop and try another exercise from the list below.
Cat-Cow
How it works: One of the most commonly performed herniated disc exercises is this one. The cat-cow stretch, which opens the intervertebral disc space and combines two yoga poses, can help release pressure on the herniated disc. Additionally, it increases spine mobility, which may lessen disc herniation discomfort and accelerate recovery.

How to do it: To begin this exercise, get down on your hands and knees. Breathe deeply and allow your stomach to “drop” toward the floor as you gaze up at the ceiling.
– Then exhale, slowly turn your back, place your hands on the floor, and bend your neck just enough to see your feet above.
– Try to complete 10 repetitions of this stretch in two to three sets.
Bird Dog
How it works: This is a great technique to strengthen your lumbar back muscles and core.
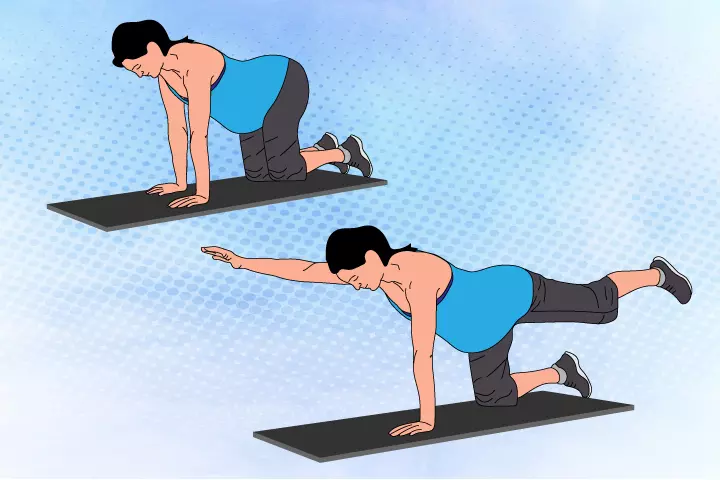
How to do it: Start on your hands and knees, placing your knees beneath your hips and your hands beneath your shoulders.
– Before starting any movement, brace (contract) your core as firmly as you can.
– Lift your left arm and reach it forward until it is in line with your chest while bracing your core. Kick your right leg backward until it is in line with your torso, likewise.
– When doing this, it’s crucial to avoid arching your lower back.
– Return to the starting position cautiously after holding this position for two to three seconds.
– Repeat with your left leg and right arm.
– For ten repetitions, switch sides. Avoid arching your lower back, and just stretch your arms and legs as far as is comfortable.
Plank
How it works: This is a great exercise to develop your gluteal muscles and deep core.
How to do it: To begin, lie on your stomach with your forearms resting against the mat.
Use your core to elevate your body so that you can rest on your forearms and toes.
– Maintain a neutral spine, which means your butt shouldn’t be elevated in the air or sagging in the low back. Lower it to the floor after maintaining the plank position for 20 to 30 seconds.
– Make an effort to complete this exercise two to five times.
** Throughout the entire workout, make sure your back stays straight.
Stretches for a lumbar herniated disc
Hamstring Stretches for Improved Flexibility
People who suffer from lower back pain frequently have tight hamstrings. Regular hamstring stretching dramatically lowers pain and disability in patients with lumbar radiculopathy caused by herniated discs, according to a study published in the Journal of Physical Therapy Science.
How to do it: Sit on the floor with one leg bent and the other extended to stretch your hamstrings.
With both hands, reach forward toward the outstretched foot until a slight stretch is felt.
Repeat on the opposite side after holding the stretch for 20 to 30 seconds.
Piriformis Stretches for Relieving Sciatic Nerve Pressure
Sciatic nerve constriction and pain can be worsened by piriformis muscle tightness. In individuals with lumbar disc herniation, piriformis stretching can enhance functional outcomes and reduce sciatic nerve discomfort.

How to do it: Stretch the piriformis by bending both knees while lying on your back.
Pull the opposing knee softly toward your chest after crossing one ankle over it.
After 25 to 30 seconds of holding the stretch, switch sides.
Quadriceps and Hip Flexor Stretches for Reduced Strain
The lower back may be further strained by tight hip flexors and quadriceps. People with low back pain, especially those with herniated discs, may have less pain and handicap if they regularly stretch these muscles.
How to do it: Place your feet hip-width apart and stand to stretch these muscles.
Feel a stretch in the front of your thigh as you grab one ankle and pull it toward your buttocks.
Repeat on the opposite side after holding the stretch for 20 to 30 seconds.
Low-impact cardiovascular exercises for a lumbar herniated disc
Safe aerobic exercises are essential for strengthening the heart without making a herniated disc worse.
- Walking & exercises for brisk walking
Walking is an accessible, low-impact exercise that can help people with herniated discs heal and improve their cardiovascular fitness. Walking can be a beneficial form of exercise for those with persistent low back pain, according to a meta-analysis, improving their quality of life and physical function.
Begin with short walks and progressively increase the length and speed over time. - Stationary Biking and Cycling for Lower Body Exercise
- Cycling is an additional low-impact exercise that reduces spinal strain. People with low back pain have been shown to benefit from stationary bikes, which increase both functional ability and pain intensity. Think about riding a bike on a flat surface outside or utilizing a stationary bike.
- Water-Based Activities to Increase Buoyancy and Decrease Impact
Swimming and water aerobics are examples of water-based workouts that provide buoyancy, which lessens the strain on the joints and spine. According to a JAMA Network study, people with persistent low back pain, particularly those with herniated discs, can benefit from aquatic training in terms of both pain and physical function. Engage in water-based activities for a mild yet efficient cardiovascular workout.
Posture correction and alignment exercises for a lumbar herniated disc
Corrective exercises can greatly lessen lower back pain by encouraging good posture and spinal alignment.
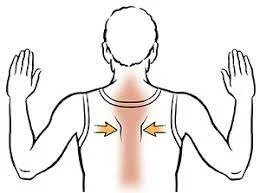
Upper Back Support with Shoulder Blade Squeezes
- Shoulder blade squeezes improve posture and lessen lower back strain by strengthening the muscles surrounding the upper back. Long-term low back pain sufferers may benefit from scapular stability exercises.
- To do shoulder blade squeezes, sit or stand with your shoulders relaxed and your back straight.
- Act as though you are holding a pencil between your shoulder blades.
- After 5–10 seconds of holding the squeeze, let go and do it again.
Squats and Wall Sits for the Best Spinal Alignment
Squats and wall sits work the lower body and core, which improves spinal stability and alignment. Squats are a good way to work your lower back extensors and abdominal muscles.
To execute wall sits:
- Place your feet shoulder-width apart and lean your back against a wall.
- Bend your knees to a 90-degree angle and slide slowly down the wall.
- Maintain the posture for 20 to 30 seconds, then go back to your feet.
Yoga and Pilates for Posture Improvement
- Exercises that improve posture, flexibility, and core strength are incorporated into yoga and Pilates.
- People with persistent low back pain, particularly those with herniated discs, can greatly lessen their pain and handicap by practicing yoga.
Exercise Progression and Gradual Intensity Increase
- For people with herniated discs, we stress the significance of monitoring exercise intensity and implementing cautious progression. Start with easy workouts that don’t hurt, and as time goes on, progressively get more difficult and intense.
- Strengthening muscles and increasing spinal stability are two advantages of resistance exercise. To prevent making the issue worse, resistance training must be done safely and under the supervision of a fitness expert or physical therapist.
- During and after exercise, pay special attention to your pain levels and listen to your body. Avoid or alter a workout if it makes you uncomfortable or aggravates your problem.
Exercises to Avoid
- Activities with a High Impact
High-impact exercises like running and jumping can strain the spine and make a herniated disc worse. The spinal discs are under a lot of stress from these activities, which raises the possibility of additional harm and discomfort. - Excessive Weightlifting
Your lower back may experience undue strain when lifting heavy weights, especially if you do it in an incorrect manner. Avoid heavyweight workouts that can worsen a herniated disc, such as overhead presses, squats, and deadlifts. - Rotating Motions
Exercises that cause the spine to twist, like yoga positions or Russian twists, might make a herniated disc worse. These motions may worsen pain and put more strain on the damaged disc. - Forward Bends and Toe Touches
Toe touches and forward bends are examples of bending forward from the waist, which can put excessive strain on the lower back. These motions might increase pain and suffering and worsen a herniated disc. - Crunches and Sit-Ups
Conventional crunches and sit-ups can put more strain on the lumbar region. Flexing the spine during these workouts can worsen a herniated disc. Choose activities that strengthen your core without putting undue strain on your back, like planks.
MCEs (stabilization/core stability exercises)
These therapeutic exercises are frequently recommended for patients who have a disc herniation.
- Intended to retrain the diaphragm, pelvic floor muscles, gluteals, paraspinals, and abdominals to co-activate.
- The primary biological basis for MCEs is the concept that people with LBP have impaired spinal stability and control.
- The program starts with the understanding that the mid-range between lumbar flexion and extension range of motion is the spine’s natural position and is thought to be the position of power and balance for enhancing performance in a variety of sports.
- MCEs must first engage in low-level, prolonged isometric contraction of the trunk-stabilizing muscles and then gradually incorporate them into functional tasks.
- MCE is often administered in one-on-one supervised treatment sessions, and it occasionally incorporates ultrasound imaging, palpation, and/or pressure biofeedback units to give feedback on trunk muscle activation.
- In patients with lumbar disc herniation, a core stability program improves functional status, lowers pain levels, and increases trunk muscle static endurance. Stabilization exercises are more beneficial than no treatment, according to moderate evidence from individual high-quality trials.
General rules for exercise/ dos and don’ts
- Take your time exercising. Maintain the exercise position for five slow counts. Work your way up to 10 repetitions, starting with 5. In between the repetitions, fully relax.
- Spend ten minutes exercising twice a day.
- Exercise, which can cause pain, should be done with caution.
- Make sure to work out every day.
Physiotherapy modalities and their use in disc herniation
- Stretching: According to low-quality research, incorporating hyperextension into an intense exercise program may not improve functional status or pain outcomes more than intense exercise alone. Additionally, no statistically significant or clinically relevant differences in pain and impairment were observed between strength training and stretching together versus strength training alone.
- Strengthening your muscles will help you manage discomfort and provide a strong support system for your spine. Strength and power can be practiced once core stability has been completely restored and is under control. However, it is only essential if it is for the patient’s functioning or activities. Because of the combination of its two components—force and velocity—this power must be avoided when performing the core stability exercises. This combination increases the likelihood of developing back discomfort and issues.
- Manipulative Treatment: For lumbar disc herniation, manipulative treatment looks to be safer, more effective, and superior to other forms of therapy. However, more research is required to gather high-quality evidence.
- Traction: According to a recent study, patients with intervertebral disc herniation benefit from traction therapy in terms of pain, disability, and SLR. Additionally, one study discovered some extra advantages to combining mechanical traction with electrotherapy and medication.
- Aquatic Vertical Traction: Compared to entering a supine flexing posture on land, this approach showed stronger effects on spinal height, pain relief, centralization response, and pain severity in individuals with low back pain and symptoms of nerve root compression.
- Cryotherapy: Because it lessens pain and inflammation, cryotherapy is employed.
- Ultrasound: Ultrasound increases blood flow to the damaged area by stimulating it with sound waves. In the US , it increases the extensibility of connective tissues.
- Transcutaneous electrical nerve stimulation (TENS): This technique encourages mild relaxation.
- Laser therapy: Laser therapy improves mobility, reduces discomfort, and speeds up the healing process.
- Hot Therapies: may provide heat to the target location to improve blood flow. Blood provides additional oxygen and nutrients, which aid in the healing process. Additionally, blood eliminates waste products from muscular contractions.
- Interferential therapy: The goal of interferential therapy is to lessen inflammation and pain.
- Shortwave diathermy: continuous SWD in chronic conditions and pulsed SWD in acute conditions.
Post-surgical treatment
Your healing following spine surgery is greatly aided by postoperative therapy. It helps you rebuild strength, flexibility, and endurance in addition to easing pain and suffering, allowing you to return to your regular activities as quickly as possible.
A rehabilitation team’s supervision can also aid in avoiding possible side effects like infections, blood clots, and muscle weakness. Recall that the purpose of postoperative rehabilitation is to empower you on your path to regaining your independence as well as to promote healing.
Why is physiotherapy important after spine surgery?
- Restoration of Function and Movement: Temporary mobility restrictions may result from the surgical procedure. Through focused exercises, physiotherapy aids in the restoration of these motions.
- Complication Prevention: Post-operative problems, including stiffness, muscle atrophy, or blood clot formation, can be prevented with the aid of physiotherapy.
- Pain Management: Physiotherapy methods, including massage, exercises, and heat or cold therapy, can effectively control postoperative pain.
- Improving Quality of Life: Physiotherapy can greatly improve the quality of life following surgery by increasing mobility and lowering discomfort.
Timeline of physiotherapy after spine surgery
Initial Post-Operative Period (The Initial Days)
- The main objective in the initial days after your spine replacement procedure is to control pain and suffering. Your physiotherapist and doctor will collaborate closely to make sure you are comfortable and to encourage you to start with easy movements right away.
Here, a few crucial tasks could be:
- To avoid blood clots, move your legs and feet gently.
- Moving on to supported sitting on the bed’s edge.
- Attempting quick walks under your physiotherapist’s guidance.
- Remember that each patient’s road to recovery is different, and these exercises will be modified according to your comfort level and skill level.
Phase of Early Rehab (First 2-4 Weeks)
- As the early stages of rehabilitation begin, the emphasis switches to increasing muscle strength and mobility. Starting with aided walking, you will progressively increase the distance each day.
Physiotherapy during this time may include:
- Exercises to improve the strength of your spine-supporting core muscles.
- Improving coordination and balance to avoid falls.
- Instructions for protecting your new spine while standing, sitting, and moving.
Phase of Intermediate Rehab (4–12 Weeks)
- Regaining your independence will be the main focus as you go into the intermediate phase of therapy. In order to achieve total fitness, your physiotherapist will help you increase the intensity of your exercise regimen.
During this phase, important activities include
- Walking farther on foot without assistance.
- Beginning with easy leg and upper body strengthening exercises.
- Introduction of stationary cycling and other mild aerobic workouts.
Phase of Advanced Rehab (3-6 Months)
- The goal of the advanced rehabilitation phase is to get you back to your regular activities. Your workout regimen will now be more comprehensive, emphasizing the development of your strength, flexibility, and endurance.
At this point, possible activities include:
- Advanced strengthening activities with light weights or resistance bands.
- Gradual return to hobbies and leisure pursuits.
- Routine examinations with your physician to evaluate the health of your spine.
Extended Rehab (6 Months and Up)
After six months, the long-term phase of therapy finally starts. You ought to have recovered the majority of your strength and range of motion by now. Here, keeping yourself physically active and avoiding further spinal issues are the major goals. Depending on your development, your physiotherapist may introduce new exercises as you continue the ones you learned in earlier periods. At this point, maintaining a long-term healthy lifestyle is essential for both your general health and the lifetime of your spine replacement.
Types of physiotherapy exercises after spine surgery
Exercises for Range of Motion
Your physician may recommend range-of-motion exercises as part of your recovery. The term ‘range of motion’ here refers to a joint’s entire range of motion, often its range of flexion and extension. The purpose of these workouts is to preserve and enhance your spine’s and the surrounding muscles’ range of motion and flexibility. Usually beginning with basic exercises like neck or lower back tilts and rotations, they progressively advance to increasingly difficult ones as your strength and stamina increase.
Exercises for Strength Training
Strengthening the muscles that support your spine is just as important as regaining your flexibility. By focusing on these areas, strengthening exercises improve stability and lower the chance of further accidents. Under the guidance of a qualified physiotherapist, they could involve exercises like pelvic tilts or leg raises. The saying “slow and steady wins the race” is especially applicable in this situation because pushing yourself too hard can cause stress or discomfort.
Exercises for Proprioception and Balance
The term ‘proprioception’ here describes the body’s awareness of its position, motion, and activity. It is what allows us to walk freely without being aware of our surroundings. After surgery, these exercises aid in the recovery of your balance and spatial awareness. They could entail walking heel-to-toe or standing on one leg, which are exercises that test your balance and develop your proprioception.
The aerobic conditioning
The importance of aerobic conditioning in the healing process cannot be overstated. It strengthens your heart, expands your lungs, and improves your general endurance. Commonly advised activities include swimming, cycling, and walking. Always remember to begin these workouts slowly, then progressively increase the duration and intensity to match your body’s rate of recovery.
Functional training
Not to be overlooked is functional training. This includes workouts that make it easier for you to carry out everyday tasks. After surgery, functional training helps you restore your independence in daily activities, such as getting out of a chair and picking up items from the floor.
Tips for successful physiotherapy after spine surgery
- Attend Physiotherapy Sessions Frequently: Your physician will arrange for a number of appointments with a qualified physiotherapist. Attending these regularly is essential because missing sessions can hinder your growth.
- Observe the directions. With diligence, you will learn particular workouts from the physiotherapist that are suited to your recovery requirements. To prevent issues, make sure you follow instructions precisely.
- Continue to Communicate Openly: Tell your therapist right away if you feel any pain or discomfort throughout the session. The exercise can then be modified to fit your comfort level.
- Drink Plenty of Water and Eat Healthily: During the recovery phase, adequate hydration and nutrition are essential. Eat a well-balanced diet that is high in fiber and protein, as these nutrients aid in tissue repair.
- Maintain Your Positive Attitude: Recovery can be emotionally and physically exhausting. Keep an optimistic outlook and have faith in the process. Keep in mind that you are one step closer to having a healthier spine.
Prevention
- Good posture. Maintain a straight posture by aligning your neck and shoulders. Think of your spinal column as a tool that must always be used properly. Your spine becomes unstable if you slouch, tilt your neck forward to text, or sit at a desk with poor posture all day.
- Make your core stronger. Your spine is shielded from damage by the core muscles, which are found in the middle of your body. Regularly performing exercises like planks with proper technique can help protect the spinal column.
- Lift properly. You must always maintain proper form when bending to pick up something, even if it’s a light object. Avoid bending at the waist. Rather, lift as though performing a squat while bending at the knees and maintaining a straight back.
- Quit smoking. A herniated disc can result from disc degeneration, which nicotine has been shown to contribute to. Smoking is hazardous to your back in addition to your lungs.
- Put on appropriate footwear. Since everybody is unique, make sure your shoes provide the proper amount of support. To find the ideal shoes, specialty shoe retailers will fit and test your feet. Try to avoid high heels and sit down whenever you can.
- Maintain a healthy weight. It’s a reality of life that carrying extra weight puts additional strain on your spine. Maintaining a healthy weight, exercising, and eating well will relieve stress on your spine and reduce the risk of developing a herniated disc.
- Make stretching a priority. Every muscle in your body has some sort of connection to your spinal column. Stretches like hamstring and hip stretches should be prioritized because they will relieve strain from tense muscles and maintain the alignment and health of your spine.
Conclusion
Unless there is significant neurological damage, conservative treatment should be the first line of treatment. Surgery is typically reserved for extreme cases since its outcomes are not always foreseeable. Following surgery, patients frequently experience worsening neurological impairments and lingering discomfort. For the majority of patients, physical treatment is essential. Although there are many variables that affect the results, people who engage in regular exercise and keep their weight in check fare better than those who lead sedentary lives.
One of the most prevalent conditions that causes individuals to have leg and/or low back pain is intervertebral disc herniation. It frequently happens as a result of the annulus fibrosus degenerating with age. Seventy-five percent of intervertebral disc herniations heal on their own within six months, and disc herniations are typically asymptomatic.
Different levels of the spine might experience disc herniation. The lumbar discs between vertebrae L4-L5 and L5-S1 are most frequently affected by a herniated disc. Compared to lumbar disc degeneration, cervical disc herniation is less common. Levels C5–C6 and C6–C7 are where the cervical disc herniation is most commonly found. stability exercises)
FAQs
What is the primary cause of a disc herniation?
The most frequent cause of disc herniation is a degenerative process where the nucleus pulposus weakens and loses hydration with age. A progressive disc herniation that may result from this process may cause symptoms. Trauma is the second most common cause of disc herniation.
What other names are there for a herniated disc?
A piece of the disc nucleus that is forced out of the annulus and into the spinal canal by a tear or rupture in the annulus is known as a herniated disc (also called bulged, slid, or ruptured). Herniated discs are typically in the early stages of degeneration.
What occurs if treatment for a herniated disc is not received?
In certain situations, this injury may cause permanent disability if treatment is delayed. Your cervical spine may be the source of arm or leg pain if you have a little herniation close to a nerve root. When you turn your head, herniated discs close to the middle of your spine might also hurt your neck and back.
How can a herniated disc be avoided?
Maintaining proper posture, exercising frequently to strengthen your back and core muscles, lifting heavy objects with your legs, keeping a healthy weight, and quitting smoking are all ways to avoid a herniated disc. Additionally, it’s critical to avoid extended periods of sitting by moving around frequently and sleeping in a position that supports your spine.
What is the prevalence of herniated discs?
Nearly 35% of people currently have herniated or bulging discs, many of which are asymptomatic, according to recent studies.
References
- Crna, R. N. M. (2023, March 15). Slipped (Herniated) disc. Healthline. https://www.healthline.com/health/herniated-disc
- Disc Herniation, Physiopedia, https://www.physio-pedia.com/Disc_Herniation
- Stretanski, M. F., Hu, Y., & Mesfin, F. B. (2025, September 14). Disc Herniation. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK441822
- Herniated disk: MedlinePlus Medical Encyclopedia. (n.d.). https://medlineplus.gov/ency/article/000442.htm
- Barrow Neurological Institute. (2025, September 19). Herniated disc – Symptoms, diagnosis, treatment. https://www.barrowneuro.org/condition/disc-herniation/
- Härtl, R., MD. (2024, February 28). Diagnosing a lumbar herniated disc. Spine-health. https://www.spine-health.com/conditions/herniated-disc/diagnosing-lumbar-herniated-disc
- Physiotutors. (2022, August 10). Bowstring Test | Radicular Pain Assessment | Radicular Syndrome. https://www.physiotutors.com/wiki/bowstring-test/
- Prone Knee Bend test. (n.d.-b). The Student Physical Therapist. https://www.thestudentphysicaltherapist.com/prone-knee-bend-test.html
- Forsthoefel, C., MD. (n.d.). Lumbar disc herniation – spine – orthobullets. https://www.orthobullets.com/spine/2035/lumbar-disc-herniation
- Herniated disk in the lower back – OrthoInfo – AAOS. (n.d.-b). https://orthoinfo.aaos.org/en/diseases–conditions/herniated-disk-in-the-lower-back/
- PharmD, J. C. (2019b, October 25). What to know about herniated disc surgery. https://www.medicalnewstoday.com/articles/326780#recovery-process-and-timeline
- What are the 4 stages of degenerative disc disease? – Spine surgery. (2024, April 2). Spine Surgery. https://www.spine.md/insights/stages-of-degenerative-disc-disease
- Freutel, N. (2023, May 30). Neck exercises and stretches for a herniated disc. Healthline. https://www.healthline.com/health/fitness-exercise/herniated-disk-exercises
- Null. (n.d.-c). What is Herniated Disk? Symptoms, Causes, Diagnosis & Physiotherapy Treatment of Herniated Disk or Slipped Disc. – CB Physiotherapy. Cbphysiotherapy. https://cbphysiotherapy.in/condition/herniated-disk-or-slipped-disc
- Mitchell, G. (2024, August 15). Five Safe Exercises for Herniated Disk Back Pain | NJ Spine & Ortho. NJ Spine & Orthopedic. https://www.njspineandortho.com/safe-exercises-for-herniated-disk-back-pain/
- McQuilkie, S., DC. (2023b, July 3). 7 Herniated disc exercises for lower back (Lumbar area). PostureFlow (Formerly Back Intelligence). https://backintelligence.com/herniated-disc-exercises/
- Das, D. K. (2025, June 12). Physiotherapy after spine surgery – Pristyn Care. Pristyn Care. https://www.pristyncare.com/blog/physiotherapy-after-spine-surgery/
- Pneuma. (2025b, June 20). Healing from Herniated Disc: Effective Exercises For Herniated Disc in Lower Back – Mainstay Medical. Mainstay Medical. https://mainstaymedical.com/exercises-for-herniated-disc-in-lower-back
- Herniated Disc: 7 Ways to Help Prevent it from happening | National Spine Health Foundation. (2023, February 1). National Spine Health Foundation. https://spinehealth.org/article/herniated-disc-5-ways-help-prevent-it-from-happening/




27 Comments