

Cervical spondylosis: Cause, Symptoms, Diagnosis, Treatment, Exercise
What is the meaning of cervical spondylosis?
Cervical spondylosis is also known as neck arthritis.
It is age-related wear and tears affecting the cervical spinal disc in your neck.
As the disc dehydrates and shrinks, signs of osteoarthritis develop, including bone spurs. Cervical spondylosis is a common condition and the risk increase with age.
This condition is present in more than 90% of people aged 60yrs and older.
Too many people have it but never experience symptoms. some people who have it can do routine activities.
Cervical spondylosis usually doesn’t lead to disability. But sometimes these changes in the spine can irritate or impinge the spinal cord or nerve roots because of that you may feel discomfort in the neck region. This can cause your legs or hands to feel weak or clumsy.
Anatomy of the cervical spine
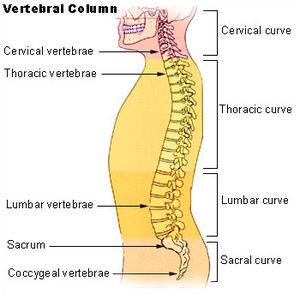
The cervical spine is an important one anatomically, clinically, and therapeutically.
It is the region where the nerves of arms arise through the brachial plexus and where the cervical plexus forms providing innervation to the diaphragm surrounded by other structures.
It also allows the opening of important vascular structures to reach the brain and allows an attachment area for muscles that move the head, neck, and shoulder girdle.
To understand this complicated region, we will consider the bony structures first, and then discuss the ligaments, nerves, and musculature that are associated with this region of the cervical spinal column, coming to the conclusion with some clinical implications of damage to some of these structures.
Types of vertebrae
- Typical (C3-C6)
- Atypical (C1, C2, C7)
Structure of typical vertebrae
- Vertebral body
- Transverse process
- Spinous process
- Vertebral foramen
- Vertebral arch
- Articular processes
Intervertebral discs
The vertebral column protects the spinal cord which runs through its central cavity.
Between vertebrae, there is an intervertebral disc that is filled with a gelatinous substance known as nucleus pulposus, which provides cushioning to the spine and is surrounded by annulus fibrosis. They allow the vertebrae to move and work as shock absorbers.
Ligaments
- The ligaments of the cervical spine are a combination of ligaments that continue from the lower regions of the vertebral column and ligaments that are unique to the cervical spine.
- Anterior longitudinal ligament (ALL)
- Posterior longitudinal ligament (PLL)
- Ligamentum flavum
- Intertransverse ligament
- Interspinous ligament
- Nuchal ligament
- Alar ligament
- Apical ligament
- Transverse ligament
Nerves
Cervical plexus and brachial plexus
Many important nerves arise from the cervical spinal cord.
Most of these nerves originate in one of two plexuses: The cervical plexus or The brachial plexus
Cervical plexus
It arises from the anterior rami of the spinal nerves associated with C1-C4 (some texts include the C5 nerve root).
The cervical plexus lies deep to the sternocleidomastoid (SCM) muscle and anteromedial to the levator scapulae and middle scalene muscles.
The branches of this plexus can be categorized as either muscular or cutaneous.
Muscular branches
- Phrenic nerve(C3-5): It supplies the diaphragm.
- Ansa cervicalis (C1-3): It supplies the infrahyoid muscles.
- Suboccipital Nerve (C1): It supplies the suboccipital muscles.
- Nerves roots of C1-C3: It supplies the prevertebral muscles.
The cervical plexus also contributes branches to these two nerves:
Dorsal scapular (C4,5): It supplies the rhomboid major and minor, and levator scapulae muscles.
Long thoracic (C5-7): It supplies the serratus anterior muscle.
Cutaneous branches
- Lesser occipital (C2): It supplies the skin of the neck and scalp.
- Great auricular (C2,3): It supplies the skin surrounding the ear.
- Transverse cervical (C2,3): It supplies the skin over the anterior cervical region.
- Supraclavicular (C3,4): It supplies the skin over the clavicle and shoulder.
Brachial Plexus
Brachial plexus arises from the anterior rami of the spinal nerves associated with C5-T1 where the nerve roots appear between the anterior and middle scalene muscles.
The nerve roots instantly combine to form nerve trunks:
C5-C6 nerve roots form the upper trunk
C7 nerve root from the middle trunk
C8-T1 nerve roots form the lower trunk
Each trunk divides into divisions: Anterior division
Posterior division
Divisions combine to form three cords:
- The lateral cord
- The medial cord
- The posterior cord
- The cords combine to form the five major nerves that supply the majority of the upper limb.
Musculocutaneous (C5-7): It supplies muscles of the anterior compartment of the arm, and the skin of the lateral forearm.
Median (C5-8, T1): It supplies the majority of the muscles in the anterior compartment of the forearm, and the skin of the lateral 3-and-a-half fingers (mostly palmar aspect) and palm.
Ulnar (C8, T1): It supplies the majority of the intrinsic muscles of the hand, and the skin of the medial 1 and a half fingers and hand (palmar and dorsal aspects).
Radial (C5-8, T1): It supplies all muscles in the posterior compartments of the arm and forearm, and the skin of lateral 3 and a half fingers (dorsal aspect).
Axillary (C5,6): It supplies the deltoid and teres minor muscles, and the skin over the deltoid.
Also, several minor nerves arise from the brachial plexus. The dorsal scapular nerve and long thoracic nerve mentioned previously, these minor nerves are the:
Nerve to subclavius (C5,6): It supplies the subclavius muscle.
Suprascapular (C5,6): It supplies two of the rotator cuff muscles (the supraspinatus and infraspinatus).
Lateral pectoral (C5-7): It supplies the pectoralis major muscle.
Medial pectoral (C8, T1): It supplies the pectoralis major and pectoralis minor muscles.
Medial cutaneous nerves of the arm and forearm (C8, T1): these supply the skin of the medial aspect of the arm and forearm.
Thoracodorsal (C6-8): It supplies the latissimus dorsi muscle.
Upper and lower subscapular (C5,6): Together they supply one of the rotator cuff muscles, the subscapularis muscle.
The teres major and teres minor muscles are supplied by the lower subscapular nerve.
Muscles attached to the cervical spine
Most of the muscles in the cervical region are not attached to the cervical spine, but many of them attach to the cervical spine. The following muscles originate or insert (at least partially), or both, onto the vertebrae in the cervical spine. If a muscle attaches to the skull it will move the head, if a muscle does not attach to the skull then it will only move the neck.
Anterior neck muscles which flex the head, flex the neck, and elevate ribs 1 and 2
Rectus capitis anterior
Rectus capitis lateralis
Longus capitis
Longus colli
Anterior scalene
Middle scalene
Posterior scalene
Superficial back muscles that extend the head and neck, elevate and retract the scapula, and elevate ribs:
Trapezius
Levator scapulae
Rhomboid minor
Serratus posterior superior
Suboccipital muscles that extend and rotate the head:
Rectus capitis posterior major and minor
Obliquus capitis superior and inferior
Deep back muscles
spinotransversales muscles which extend the neck, and rotate the head:
Splenius capitis
Splenius cervicis
Erector spinae muscles that extend the neck and head:
Iliocostalis muscle
Iliocostalis cervicis
Iliocostalis thoracic
Longissimus muscle
Longissimus capitis
Longissimus cervicis
Spinalis cervicis
Transversospinalis muscles which extend the neck, extend and rotate the head:
Semispinalis capitis
Semispinalis cervicis
Semispinalis thoracic
Multifidus
Rotatores cervicis
Epidemiology
According to NCBI (National Center for Biotechnology Information), the prevalence of cervical spondylosis was 13.76%, although it differed significantly among the urban, suburban, and rural populations (13.07%, 15.97%, and 12.25%, respectively). Moreover, it was higher in females than in males (16.51% vs 10.49%). The prevalence among different age groups had a reverse U shape.
Pathophysiology
Cervical spondylosis is the result of disc degeneration or bony projections along the edges of bones(bone spurs). As discs age, they fragment, lose water and shrink. First, it starts in the nucleus pulposus of the disc. This results in the central annular lamellae becoming distorted inside while the external concentric bands of the annulus fibrosis bulge toward the edge of the vertebrae.
Because of this increased mechanical stress on the cartilaginous end plates at the vertebral body lip.
Subperiosteal bone formation occurs after that, forming osteophytes bars that extend along the anterior aspect of the spinal canal and, in some cases, irritate the nerve tissue. These most likely stabilize adjacent vertebrae, which are hypermobile as a result of the lost disc material.
Can cervical spondylosis affect the brain?
The National Library of Medicine did a study on it.
It suggests that patients with cervical spondylosis may present anatomical and functional adaptive changes in the brain. Cervical spondylosis may lead to white matter damage, gray matter volume loss, and functional adaptive changes in the sensorimotor cortex. The result of this study reported in this work may be of value to better understanding the effect of prolonged cervical spine compression in the brain.
Who is more prone to getting cervical spondylosis?
Aging is a major factor in cervical spondylosis. In older age, the vertebral space becomes narrow and discs between the vertebrae become less spongy so the cushioning is almost gone. Ligaments get thicker and impinge in the space of the spinal canal.
Previous injury to the neck. People in certain occupations or who perform specific activities — such as construction workers, weight lifters, and other athletes may put more stress on their necks.
Poor posture also plays a role in the development of spinal changes that result in cervical spondylosis.
In addition to age, you are more likely to experience neck pain symptoms related to cervical spondylosis if you:
Smoke cigarettes or used to.
Have any family members with this condition.
Strain your neck frequently for your job, like looking overhead (for example, painters) or downward (plumbers or flooring installers) for many hours every day or keeping your head in an inappropriate position for a longer time (for example, staring at a computer screen that is too high or low).
Have a previous neck injury, such as from any road traffic accident.
Are exposed to a lot of vibrations like drivers.
What causes cervical spondylosis?
As you get older, your spine goes through some changes because of normal wear and tear.
In the middle of your age, the discs between your vertebrae start to change.
These changes can include:
Degeneration
The spinal discs in your neck may slowly degenerate(wear down). With time, the discs become thinner, and the soft tissue becomes less elastic. If you or your parents measure in a little shorter in height than you did years ago, this is normal settling of your discs.
Herniation
Normal aging can cause part of your spinal disc to tear or crack which is known as a herniated disc. The herniation can allow the disc to pop out and irritate nearby tissue or a spinal nerve. This pressure/discomfort can cause pain, tingling, or numbness.
Osteoarthritis
It is a progressive condition that causes degeneration of cartilage in your jopints (wear-down with time).In osteoarthritis, cartilage degenerates faster than in normal aging.
Bone spurs
When cartilage in the vertebral joints starts to degenerate so the bone tissue rubs against other bone tissue and abnormal bony growths develop on joints of the vertebral edges. These abnormal bony growths are called osteophytes or bone spurs. These are common as your age. Often, they cause no symptoms.
Symptoms
Symptoms of cervical spondylosis can include:
Cervical radiculopathy:-
Neurological deficits (problems with reflexes, sensation, or strength). It may be experienced in the arm due to nerve root compression. Cervical radiculopathy may also be accompanied by radicular pain.
What Is Cervical Radiculopathy?
The trouble with gripping or lifting objects. This problem can happen if numbness or weakness goes into the arm and fingers.
Sometimes the patient feels headaches. Because of discomfort irritation in the neck can affect muscles and nerves connected to the head.
Radicular pain:- This pain can radiate along a nerve from the neck into the shoulder and arm. This nerve pain might feel like it is burning or searing.
When you move your neck you feel an abrasion.
Sharp pain:
The patient feels stabbing-like pain. This pain localized to one spot. This type of pain typically occurs in the lower neck.
Stiff neck:
Difficult to move neck side by side.
General soreness around the neck region. It is described as achy, not sharp.
Problem with your balance
Difficulty in controlling your bladder or bowels
Atypical symptoms include vertigo, palpitation, nausea, discomfort in your abdomen or GI system, tinnitus, blurred vision, and hypomnesia (memory problems). Some studies have also shown that chronic neck pain has been linked to higher blood pressure.
What is cervical myelopathy?
Cervical spondylosis symptoms tend to improve with rest. Symptoms are severe in the morning and again during the night.
If cervical spondylosis results in cervical stenosis, it can put pressure on the spinal cord. This condition is known as cervical spondylotic myelopathy (CSM).
Symptoms of cervical spondylotic myelopathy include:
- Tingling or numbness and weakness in the arms and hands
- Lack of coordination and trouble in walking (feeling unsteady on your feet)
- Abnormal reflexes, Muscle spasms, and Incontinence (loss of control over bladder and bowel)
- Loss of function in hands so you may face difficulty in writing, gripping, etc.
When to Call the Doctor?
Contact your doctor if you have neck pain that intrudes into work or other routine activities.
In some cases, neck pain can be a sign of a medical emergency. Look for urgent medical care if your neck pain:
- Develops after an accident.
- If you have the sudden onset of numbness or tingling in the arms, shoulders, or legs.
- Weakness in arms and legs or loss of coordination in arms or legs.
- Neck pain includes headache, dizziness, nausea, or vomiting.
- Arises along with a stiff neck.
- Occurs with cold, fever, or unexplained weight loss.
- Does not respond to over-the-counter medications.
- Does not lessen after one week.
- This condition is the result of aging, there are treatments available that can help to reduce pain and stiffness.
- Symptoms of CSM may get worse over time. When they significantly affect your daily activities contact your doctor.
How do doctors diagnose cervical spondylosis?
Diagnosis of cervical spondylosis involves ruling out other conditions, such as fibromyalgia.
Diagnosis also involves testing for movement and ruling out the affected nerves, bones, and muscles.
For diagnosis, your doctor will start by asking some questions regarding your symptoms. Then, they’ll run through a set of some special tests.
All of this helps your doctor to rule out if your nerves and spinal cord are under too much pressure.
Your doctor will perform a physical examination to find the cause of your neck pain or other symptoms.
During a physical examination, your doctor checks your:
Neck flexibility
Muscle strength in your arms and hands.
Reflexes
How you walk(gait)
Neck and shoulder examination
Looking for trigger points (a small bump or knot in the muscle of your neck or shoulder that may be the origin of your neck pain and tenderness).
Sometimes, Doctors can diagnose cervical spondylosis with just a physical examination.
Other times, they may prefer some tests to learn more about what may be causing your symptoms.
These tests may include the following:
- X-ray: X-rays can help to know about degenerative changes to the spine (cervical spine) and problems like bone spurs.
- Computed tomography (CT): A CT scan is an imaging technology that uses multiple X-ray images to see the neck and spine in different “slices.”
- Magnetic resonance imaging (MRI): An MRI scan is used powerful magnetic and radio waves to create highly detailed images of bone and soft tissues, including those of the spinal cord.
- Electromyography (EMG): An EMG and nerve conduction study are used to check your muscles and nerves are functioning normally or abnormally. It involves the insertion of a needle into a muscle to test nerve signal speed, which can help diagnose a pinched nerve. This test takes the measurements of your nerve’s electrical activity.
- Blood tests: A complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) test can help to determine if inflammation or infection is present.
- In a myelogram, a dye injection is used to highlight certain areas of your spine. CT scans or X-rays are used to provide more detailed images of these areas.
7. A nerve conduction study checks the speed and strength of the signals sent by nerves. This is done by placing electrodes on your skin where the nerve is situated.
What are common cervical spondylosis treatments?
Cervical spondylosis does not always cause symptoms.
When your condition does cause symptoms, conservative treatments are given in most cases.
Medical treatment:
Oral medications:
Depending on how much pain you’re in, a doctor recommends a prescription of anti-inflammatory drugs like ibuprofen or naproxen sodium.
Muscle relaxants such as cyclobenzaprine can treat muscle spasms. Nerve impingement can cause severe arm pain gabapentin may reduce the pain.
Soft collar or brace:
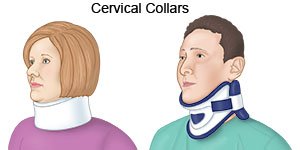
Your doctor may suggest that you wear a therapeutic collar for a short time.
It can limit neck movement and help strained muscles rest and get back to normal.
Wearing a brace for too long can lead to muscle wasting away (known as Atrophy).
Only use a soft collar or brace under the guidance of a medical professional.
Injection therapy:
Steroids can be administered to the affected area of the cervical spine.
The injection can make your symptoms better for a short period.
There are three common steroid injection procedures:
1. Cervical epidural block:
Cervical disc herniation can cause neck pain and arm pain can be treated with an injection of a combination of a steroid and anesthetic. The injection is administered into the epidural space, which is the space next to the covering of the spinal cord.
2. Cervical facet joint block:
This steroid + anesthetic injection is administered into small joints at the affected segments of the cervical spine.
3. Media branch block and radiofrequency ablation:
This procedure is used to both diagnose and treat chronic neck pain.
If pain is alleviated with an injection of an anesthetic, that spot is pinpointed for treatment.
This treatment known as radiofrequency ablation involves damaging the nerves with sound waves that are causing pain in the joint.
Physical therapy for cervical spondylosis:
Your doctor might refer you to a physical therapist for treatment.
Physiotherapy treatment can help you to stretch your neck and shoulder muscles and also help to relieve neck and arm pain.
You can try a couple of things at home if your condition is mild:
- Rest
- Take over-the-counter(OTC)pain relievers, such as acetaminophen (Tylenol) or non-steroidal anti-inflammatory drugs (NSAID), which include ibuprofen and naproxen sodium.
- Use a hot pack or a cold pack on your neck for 7-10 minutes which helps to relieve pain in your neck.
- Exercise regularly to help you recuperate faster.
- Wearing a cervical collar to limit movement and provide support
In moderate conditions, you might prefer a physiotherapist.
Pain management:
Treating Neck pain with Electrotherapy
Living with neck pain can stop you from fully enjoying and engaging with life. Unfortunately, there isn’t always an easy reply for neck pain relief. While some people respond to treatments like OTC (over-the-counter) pain medications or physiotherapy, some people may need different solutions for dealing with their pain.
Electrotherapy can be effective for pain management.
What is Electrotherapy?
Electrotherapy is a term for using mild electrical pulses to stop the pain in a point area of the body. Generally, all of these therapies use a device with electrodes to supply a low-voltage electrical current to pain areas.
The main goal of electrotherapy is pain management.
Uses of electrotherapy :
It can help improve blood circulation, which activates the body’s healing process.
This may also help to strengthen muscles, stimulate bone growth, and repair damaged tissues.
Moreover, electrotherapy may increase movement and function in an affected or stiff area.
These are low-voltage electrical currents, a person usually only senses a tingling sensation. Some people even find using electrotherapy machines to be relaxing purpose.
The side effects of electrotherapy are generally mild.
The most common side effect is patients complaining of skin irritation because of the adhesive on the electrodes. Sometimes burning sensation on the surface of the skin because of not using the device properly.
Here are common types of electrotherapy that your physiotherapist may recommend:
TENS (Transcutaneous Electrical Nerve Stimulation)
One of the most common electrotherapy devices used for pain relief. Small and sticky pads with electrodes are placed over or near the area where you sense pain. Your physiotherapist will decide the area of placement for electrodes. A series of low-voltage electrical currents are sent by the battery-operated unit to the area. You will increase or decrease the electrical current as well as the frequency and patterns of stimulation by the controller.
How do TENS work?
Generally TENS unit assists with blocking pain signals from the nerves to the brain. The change of these pain receptors can provide temporary pain relief. TENS may improve circulation and reduce muscle spasms in the neck region.
Certain TENS treatments only last for a half-hour. In some cases, you may use the TENS device for several hours at a time. You may want to keep a daily diary of your pain levels, the dosage you use, and any other symptoms that may come and go. This supports you and your physiotherapist to troubleshoot and find the best dosage for your pain relief.
PENS(Percutaneous Electrical Nerve Stimulation)
An alternative to TENS, PENS (percutaneous electrical nerve stimulation) uses needles on behalf of pads to supply electrical currents. It works as acupuncture with electrical stimulation. The benefit of using needles rather than pads means the pulse of the electrical current is closer to the pinched nerves and muscles. This can help to relieve pain immediately in some patients.
Generally, this therapy is used as an outpatient procedure. You can also use a PENS device at your home.
PEMF(Pulsed Electromagnetic Field Therapy)
It takes a different process to use electricity for pain relief. PEMF tries to heal at the cellular level rather than treating nerves or muscles. Specialized coils create an electromagnetic field around part or all of the body throughout the treatment. These electromagnetic waves stimulate the cell’s electrons assist the healing process and stimulate bone growth.
PEMF treatments can recover the cells and make them more active in healing, rebuilding, and fighting disease. Treatment is performed in a therapist’s clinic. Some PEMF products can be purchased for home use.
Cervical traction:
Cervical traction helps to relieve neck pain. It involves using weights to increase space between the cervical joints and also relieve the pressure on the cervical discs and nerve roots.
Chiropractic manipulation can help control severe pain
Other forms of physiotherapy, include the application of heat and cold therapy, traction, or exercise.
Exercises for cervical spondylosis
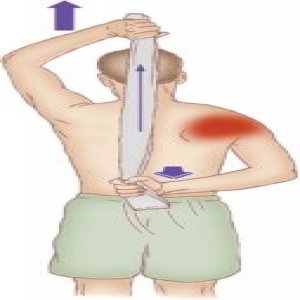
Isometric exercises for the neck:
You can perform these exercises while sitting, standing, or lying on your back.
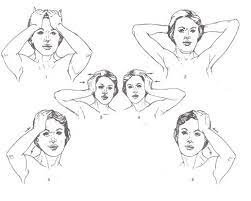
1. Cervical flexion:
Flex your neck slightly forward and place your hand on your forehead. Try to flex your head forward while pressing back with your hand.
2. Cervical extension:
Keep your neck straight and put your hands at the back of your head. Try to press your head backward while pressing forward with your hands.
3.Cervical side flexion:
Keep your neck straight and place your right hand on the right side of your head. Try to carry your head down to your right shoulder while pressing up with your right hand. Repeat the side flexion on both sides but for the left side press with your left hand.
4. Cervical rotation:
Place your left hand at chin level and turn your head slightly to the right. Place your right hand on the right side of your face. Turn your head to the right while pressing it back with your right hand. Repeat the rotation on both sides but the left side of your face with your left hand.
With specific exercises and stretches, your symptoms may relieved.
Physiotherapist focuses on stretching and strengthening your muscles and also correcting your posture.
Your physiotherapist will advise how long and how often you should practice these exercises, based on your symptoms and condition.
Stretching & exercises for cervical spondylosis
Do this stretching to help loosen tight neck and back muscles located along the thoracic and cervical spine, plus promote better good posture and upper body alignment.
You can relieve the symptoms of this condition with a few simple neck stretching exercises.
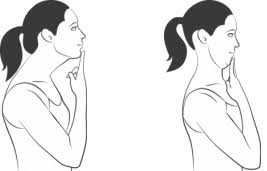
Neck stretch
Keep your body straight.
Press your chin forward in a way that stretches the throat.
Softly tense the neck muscles.
Hold this for 5 seconds.
Return to its normal position.
Press your head back with the chin held high, and hold for 5 seconds.
Carry out 5 repetitions.
Neck tilt
Tilt your head forward so that the chin comes into contact with the chest.
Softly tense the neck muscles.
Hold this for 5 seconds.
Return to its normal position.
Carry out 5 repetitions.
Neck tilt (side-to-side)
Bend your head down towards either shoulder, leading with the ear.
Softly tense the neck muscles.
Hold this for 5 seconds.
Return your head to a normal position and repeat on the other shoulder.
Carry out 5 repetitions.
Neck turn
Rotate your head to one side, being sure to keep your chin at a level height.
Tense your neck muscles for 5-10 seconds.
Return to its normal position.
Repeat on the opposite side.
Carry out 3-5 repetitions on each side.
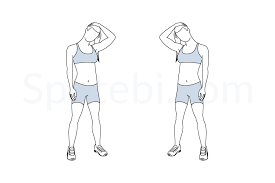
Lateral Neck Stretch
This stretching is used for the upper traps, where there is more tension. Just sit or stand in a chair with good posture (shoulders should be at back and head should be in a neutral position). Bring your left ear sideways towards your left shoulder and Keep the right shoulder relaxed. To increase the intensity of the stretch, you can anchor your right hand on the bottom of your chair or you can also extend your right arm out to the side.
Keep your upper body relaxed and pain-free and Hold for 30 or more seconds for 2-3 sets. Then, change directions.
Neck Rotation Stretch
While doing stretch pick some of the deeper sore spots in the cervical spine. Sit in a chair and with a good posture. Make sure that the neck should be in a neutral position (slightly tucked) before starting to prevent any deformities. after that, rotate your head to the right as you see over your right shoulder. When you can’t go any further, apply gentle pressure and hold and place your left hand on your cheek. Never force this stretch and always keep the neck in the neutral position.
Exercises
Exaggerated nod
The exaggerated nod counterbalances the downward and toward head position by pulling your shoulders down and back and increasing neck mobility.
How to do it:
- Sit at your desk or relax your shoulder while standing. With your mouth closed make sure your teeth touching but not clenching and look up to the ceiling.
- Stop here and open your mouth and relax your jaw. Now see if you can bring your head further back up to an inch or two.
- Keep your head fixed there and bring the lower part of the jaw to the upper part of the jaw, closing your mouth. You should feel a stretch in the front area of your neck.
Downward-Facing Dog
Downward-Facing Dog is useful for opening the front chest wall and shoulders. which are often rounded and stiffened from overuse tech usage. This is all about upper-body strength, which means if you do not have shoulder strength you might compensate by bringing your shoulders up to your ears. If you notice yourself doing this, actively put your shoulder blades down your back side, which will create space in your neck.
How to do it:
- Begin on all fours. Push your toes and lift your hips, reaching your hip bones toward the ceiling.
- Reach your heels back toward the mat, but do not let them put on the ground.
- Drop your head down so that your neck will become long. As you stay here, make sure that your wrist should stay parallel to the front side of the mat.
- To reduce the pressure on your wrists, press on the knuckles of your forefingers and thumbs.
- take at least three deep breaths and then release.
Cat-Cow
Your core and pelvis should drive the Cat-Cow flow As you inhale you create an anterior tilt to the pelvis so that your tailbone should face the ceiling, and while you exhale you create a posterior tilt so that your tailbone is facing the ground. This movement also helps increase spinal awareness, which is very important for perfect posture.
How to do it:
- Start on all fours with your shoulders over your wrists, your hips stored over your knees, and the top part of your feet pressed into the ground lengthen your head down to your tailbone to see a few inches in front of your fingers.
- To begin the ‘cat’ phase, as you exhale use your abs to curl your spine towards the ceiling while tucking in your tailbone. pull your neck and allow your chin to reach down and in, toward your chest, so you can see your ears come down by your biceps.
- To begin the ‘cow’ phase, as you inhale swoop and scoop your pelvis so your belly drops down to the floor. Widen across your shoulder blades, keep your shoulders away from your ears, and lift your chin and chest to look up towards the sky.
- Cycle through Cat-Cow a few times, keeping stress and pressure out of the head and neck.
Bow pose
It helps to counteract slouched shoulders by stretching the pectoral muscles and strengthening upper back muscles.
How to do it?
- Lie flat on your abdomen with your chin on the ground and your hand resting on either side of you.
- Bend your knees and bring your heels as close to your glutes as you can. Reach backward with both palms and grasp hold of your outer ankles. As you inhale, raise your heels toward the sky so that your chest, thighs, and upper torso elevate off the floor.
- To intensify the stretch, try to elevate your heels higher while keeping your tailbone pressed into the floor. Look forward and move your shoulders away from your ears.
- Hold this position for 10 breaths. Release an exhale by slowly lowering your thighs, and then the rest of your body, to the floor.
Chin tuck
It is a simple exercise you can do at your work, at your home. This simple stretch will help increase spinal awareness while strengthening the neck muscles to help pull your head back into alignment, says Cappo.
How to do it:
- Sit up straight in a chair and keep your chin parallel to the ground. Without leaning your head in any direction, gently draw your head and chin back, like you’re making a double chin. Be careful not to stick your head back. You should feel a stretch throughout the back of the neck.
- Now imagine there’s a string pulling your head upward like a puppet and actively elongating your neck. Actively push the base of your head away from the base of your neck. Keep your jawbone relaxed and hold this position for 3 deep breaths.
- Release your chin forward. Repeat 10 times.
These exercises can help to moderate the impact of the condition and reduce pain and stiffness. They will not cure cervical spondylosis but relieve symptoms.
These exercises may only work for less severe cases.
When Is Surgery Needed for Cervical Spondylosis?
It tends to be a chronic (long-term) condition. But in most cases, cervical spondylosis is not progressive.
Surgery is required only in some cases. The goal of surgery is to get rid of the source which pressuring the spinal cord and nerves. The surgery also gives stabilization in the form of implants or through the fusion of the vertebrae.
But surgery is required only when there is a severe loss of function.
For example, it might be required if you had a progressive loss of function in your arms and fingers. Severe spinal cord compression could result in permanent functional disability.
The surgeon can approach the cervical spine from the anterior or the posterior. Approaching from the anterior might be used to remove the discs and bone spurs causing pressure on the spinal cord. The disc was replaced with an implant. In some cases calls for the removal of both discs and parts of the vertebrae. Both discs and the vertebrae are replaced with a bone graft or implant.
Approaching from the posterior would be used to perform either a laminectomy or a laminoplasty.
There is a risk of infection and also complications with anesthesia. A rehabilitation plan usually follows surgery.
Your doctor might prescribe certain medications if OTC (over-the-counter) drugs don’t work.
These include:
steroid injections to reduce tissue inflammation
NSAIDs(nonsteroidal anti-inflammatory) drugs, such as diclofenac – to reduce inflammation
muscle relaxants, such as cyclobenzaprine
narcotics- for pain relief
anti-epileptic drugs – to relieve pain
Surgery is rarely necessary for cervical spondylosis.
How to select the proper pillow for cervical spondylosis?
The best pillow for neck and shoulder pain is firm enough to hold the head at a correct angle but soft enough to alleviate pressure points. Memory foam, latex, buckwheat, or feather pillow, as these materials provide the best balance of support and pressure relief for most people with neck pain.
1. Cervical pillows for neck pain relief
Cervical pillows especially provide neck support and keep your spine in proper posture while you’re asleep. It’s elevated where your neck is more compressed than your head lies. Your pillow should work ergonomically to support your neck. Cervical pillows come in different shapes and materials according to your comfort.
If you’re changeover from a regular pillow to a cervical pillow, you may feel discomfort for some days. Using it every day for taking a short rest during work can adapt easier.
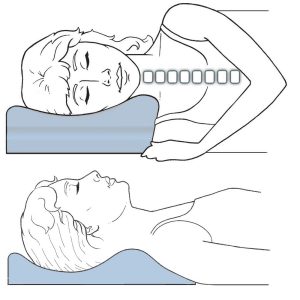
2. Pillows that mold to the neck for back sleepers
Choosing the right pillow for your neck depends on how you sleep. If you sleep on your back, try to choose a pillow that molds to your head and neck so that your neck is enough to support. Memory foam pillows or water pillows are good choices for back sleepers. They keep their shape but adjust according to your body.
3. Firm pillows for side sleepers
If you sleep on your side, then choose a firm pillow. Place the bulk of the pillow under your neck rather than your head, which provides proper support to the spine.
It helps if the pillow is elasticated. A pillow with an elasticate is one with extra material in it, with the join into rectangular panels on all four sides of the pillow so that the cushioning adjusts when you move your head. A pillow without an elasticate has only two pieces, a top and a bottom that are stitched together. Side sleepers also need to put a pillow between their legs to help maintain spine posture.
4. Thin pillows for stomach sleepers
When you’re sleeping on your stomach you put stress on your back. So, you have to use a thin pillow or no pillow to avoid stress on your back. Also, use a thin pillow under the abdominal area that can help to decrease the stress on your back.
5. Horseshoe pillows when traveling
When you’re traveling by car, plane, or train, a horseshoe pillow is a great support for your neck.
If you have neck pain, don’t let your head bend to the side when you sleep during traveling. Make sure your neck is supported
Advice:
There is no way to avoid cervical spondylosis because this condition is normal, age-related wear and tear of the joint space and disc in your neck.
Quit smoking. Smoking slows healing.
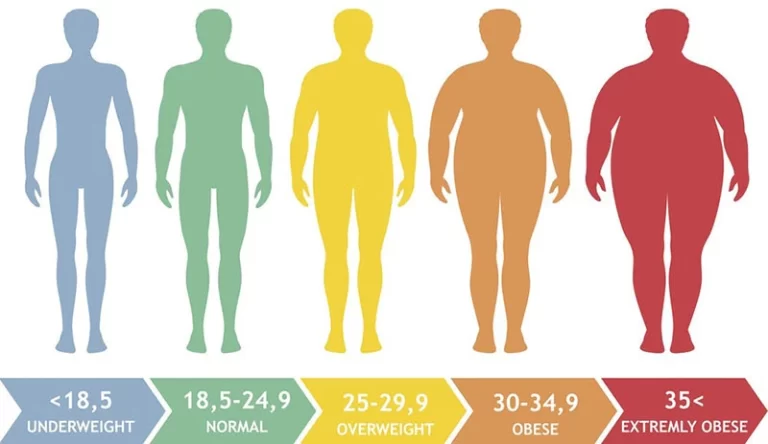
Lose weight if you are overweight.
Reduce your stress level. Walk, meditate, get a massage, try a yoga class, and exercise.
Do exercises that strengthen your neck and shoulder muscles and also do self-stretch neck muscles.
Take a short break in your work.
Always follow the instructions of your physiotherapist.

Author: Dr. Rashmi Parmar
Dr. Rashmi Parmar Physiotherapist in Mobile Physiotherapy clinic Bapunagar Branch


11 Comments