
Lumbar plexus
Introduction
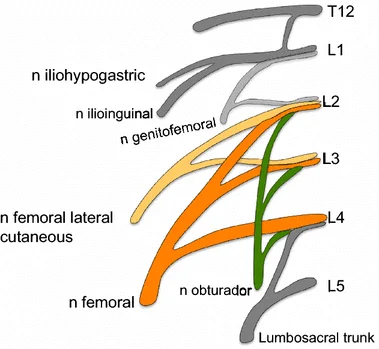
The lumbar plexus is a compound neural network formed by the lower thoracic and lumbar ventral nerve roots. They are formed where T12 to L5 leave the spinal cord through intervertebral foramina. The supply motor and sensory supply to the lower limb and pelvic girdle
The nerves get arising from the lumbar plexus are very important for the functioning of the lower extremity function and movement permitting knee extension, hip flexion, and adduction of the thigh.
Origin and Location of Lumbar plexus
The origin of the lumbar plexus is inside the psoas major muscle, anterior to the transverse processes of the lumbar vertebrae. The dorsolumbar nerve, which connects the anterior ramus of spinal nerve L1, gives to the construction of the lumbar plexus through the anterior ramus of spinal nerve T12. The iliohypogastric and ilioinguinal nerves are obtained from a single trunk formed by these roots (T12, L1). The anterior rami of L1 and L2 each have a branch that combined to form the genitofemoral nerve.
Branches and innervation of Lumbar plexus
Unlike the brachial plexus gives off various small motor muscular branches from its roots that supply the quadratus lumborum, psoas major muscle.
Branches and innervation
Unlike the brachial plexus which undergoes various clear mergers and splits, the lumbar plexus is not as uncomplicating. However, the major branches of the lumbar plexus can be arranged into groupings correlative to the psoas major muscle. These branches appear either lateral, anterior, or medial to the muscle:
- Lateral: lateral cutaneous nerve of thigh, Iliohypogastric nerve, ilioinguinal nerve, and femoral nerve
- Medial: Obturator nerve, accessory obturator nerve, and nerve to the lumbosacral trunk
- Anterior: Genitofemoral nerve
- In addition, the lumbar plexus.
Iliohypogastric nerves
The iliohypogastric nerve is formed from the anterior ramus of spinal nerve L1 but may collect a conductive branch from the anterior rami of T12. It course anterolaterally over the lower posterior abdominal wall after coming out from the superolateral border of the psoas major muscle. This nerve is a mixed nerve that gives both motor and sensory supply to the transverse abdominis and internal oblique muscle and the skin of the posterolateral gluteal surface and suprapubic area respectively.
Ilioinguinal nerve
The ilioinguinal nerve, like the iliohypogastric, gets originate from the anterior ramus of spinal nerve L1 and may also collect benefaction from the subcostal (T12) nerve. It course inferior to the iliohypogastric nerve in the same inferolateral direction. The ilioinguinal nerve is a mixed nerve and such as the iliohypogastric nerve, it gives motor supply to the internal oblique and transversus abdominis muscles. The sensory fibers of the ilioinguinal nerve supply the skin over the upper medial thigh, and skin over the portion of the external genitalia.
The lateral cutaneous nerve of the thigh
The lateral cutaneous nerve of the thigh also called the lateral femoral cutaneous nerve of the thigh, is formed by fibers of the posterior divisions of the anterior rami of spinal nerves L2 and L3. It comes out from the lateral border of the psoas major muscle and runs inferolateral to enter the iliac fossa, eventually reaching the thigh. This nerve gives sensory supply to the peritoneum of the iliac fossa and iliac fascia, and the skin of the anterior and lateral thigh (along the iliotibial tract) to the knee.
Femoral nerve
The femoral nerve is the biggest branch of the lumbar plexus and is formed from the posterior divisions of the anterior rami of spinal nerves L2-L4. It comes out from the lower lateral border of the psoas major muscle and conveys below the inguinal ligament lateral to the femoral vessels to extend the thigh. This is a mixed nerve that gives motor and sensory supply to the thigh and leg through various branches.
The femoral nerve gives motor supply to the following muscles:
- Flexors of the hip: sartorious ,pectineus ,illiacus
- Extensors of the knee: quadriceps femoris ( vastus medialis, vastus lateralis, vastus intermedius, and rectus femoris muscle)
- The femoral nerve gives sensory supply to the following areas.
- The skin of anteromedial aspect of the thigh.
- The skin of medial leg and foot region.
Genitofemoral nerve
The genitofemoral nerve get arises from the anterior rami of the spinal nerves L1 and L2. The nerve appears on the anterior surface of the psoas major muscle and course inferiorly, splitting into two branches:
The genital branch course through the inguinal canal and supplies motor fibers to the cremasteric muscle and sensory fibers to the skin of the upper anterior scrotum in males. In females, this branch gives sensory supply to the skin of the labium majus, and mons pubis
The femoral branch runs posterior to the inguinal ligament and gives cutaneous supply to the skin of the upper anterior thigh region.
Obturator nerve
The obturator nerve comes out from the medial border of the psoas major muscle and is formed from the anterior part or division of the anterior rami of spinal nerves L2-L4. This nerve is a mixed nerve that enters the medial compartment of the thigh via the obturator canal. The obturator nerve gives motor supply to the obturator externus, and adductor muscles of the hip (adductor longus, adductor brevis, adductor magnus, gracilis, and pectineus). It also gives sensory supply to the skin of the medial thigh region.
Accessory obturator nerve
The accessory obturator nerve, when present, also comes out from the medial border of the psoas major muscle. It is normally formed by the anterior rami of spinal nerves L3 and L4. This nerve supplies the pectineus muscle and the hip joint.
Nerves of the Lumbar plexus
| Nerves | segment | innervated muscle | cutaneous branches |
| ilioinguinal nerve | L1 | transverse abdominis and internal oblique muscle | anterior scrotal nerve(Male) anterior labial nerve (female) |
| iliohypogastric nerve | T12-L1 | transverse abdominis and internal oblique muscle | Anterior cutaneous ramus lateral cutaneous ramus |
| obturator nerve | L2-L4 | obturator externus muscle adduttor longus muscle adductor brevis muscle adductor magnus muscle pectineus muscle gracillis muscle | cutane4ous ramus |
| femoral nerve | L2-L4 | sartorius pectineus illiacus quadriceps femoris | Anterior cutaneous benches saphenous |
| Genitofemoral nerve | L1-L2 | cremaster in males | genital ramus femoral ramus |
| Lateral femoral cutaneous nerve | L2-L3 | Lateral femoral cutaneous |
Clinical Importance
Lumbar disc herniation
- injury to the lumbar plexus or nerves proximal and distal to it can result in different pathologies. It is very important that physical therapists have a good comprehension of the lumbar plexus in the treatment of symptomatic or indicative patients.
- Lumbar disc herniation can cause obstruction of the intervertebral foramen, compressing or impinging the lumbar spinal nerves near their entrance to the lumbar plexus. This syndrome can cause paresthesia and weakness in the lumbar plexus nerves’ supplied locations.
- The lateral femoral cutaneous nerve, which is a branch of the lumbar plexus, can lead to a common and severe nerve compression condition. This is known as meralgia paresthetica, and it occurs by the nerve becomes trapped or impinges as it passes through the inguinal ligament.
- In order to exactly determine the cause of a patient’s pain or dysfunction, first it is very important to determine which level is affected or injured. This will help in choosing the right interventions which will lead to better results.
Lumbosacral Plexopathy
Lumbosacral plexopathy is an in proportion common occurrence that can be difficult to diagnose or examine & manage. When an injury occurs to the lumbosacral plexus, patients mainly feel pain. This activity figures out the evaluation, & treatment of lumbosacral plexopathy, & highlights the role of the interprofessional team in enhancing care for patients with this condition.
The lumbosacral (LS) plexus is a network of nerves arranged by the anterior rami of the lumbar & sacral spinal cord. It is an injury to the nerves in the lumbar &/or sacral plexus. Lumbosacral plexopathy is not an unusual condition but can be very complicated to diagnose & treated. However, it is barely less frequent than brachial plexopathy. Patients with Lumbosacral plexopathy normally present with low back and leg pain. They can also involve or experience motor weakness, & other sensory symptoms of insensibility, paresthesia(numbness, tingling sensation), and sphincter dysfunction.
Lumbosacral plexopathy can be caused by multiple causes, with traumatic injury, diabetes mellitus,, neoplasms, & pregnancy being a few of the main causes. Treatment is frequently limited & varies remarkably depending on the underlying pathology.LSumbosacral plexopathy can be debilitating, severely affecting a patient’s quality or standard of life. Early recognition & management are critical in decreasing morbidity & mortality.
FAQ
What happens if the lumbar plexus is damaged?
If the lumbar plexus is damaged that leads to pain in the lower back and the leg as well as loss of sensation and weakness in all or part of a lower limb (such as the foot or calf).
Why is the lumbar plexus important?
The nerves get arising from the lumbar plexus are vital for the work of the lower extremity and regulating the ability to expand the knee, flex the hip, adduct the thigh, and much more.
What regions of the body are affected or injured by the lumbar plexus?
Lumbar plexus: abdomen, thigh, groin, Back, knees, calves. Sacral plexus: genital, thigh, calves, Pelvis buttocks, feet. Coccygeal plexus: (A small area over the coccyx the “tailbone”)
Why is the lumbar most vulnerable?
This part of the body is permitted to injury due to the large forces which must be supported, which comprise the body weight and any outer weights, as well as the forces due to the very high speed up of the body parts.
What type of bone is lumbar?
irregular bones
The lumbar vertebrae are divided into irregular bones. In truth, all vertebral bones are irregular bones. An irregular bone is a bone that does not suitable for any of the other bone groups. The other groups are flat, short, long, and sesamoid bones.
Can lumbar injury be cured?
Unfortunately, there’s no way to reverse injury to the spinal cord. But researchers are continually functioning on new treatments, comprises of prostheses and medications, that might promote nerve cell regrowth or improve the function of the nerves that persist after a spinal cord injury.
What organs are affected by the lumbar spine?
The organs that are typically associated with this type of back pain can involve.
Appendix.
Colon.
kidney
Liver.
Reproductive organs.
uterus
Gallbladder.
Abdominal aorta.
What are plexus problems?
Brachial plexus injuries (also known as Erb’s palsy and Dejerine-Klumpke’s palsy) are caused by damage to those nerves, usually from trauma, tumors, inflammation, pressure, athletic injuries, or being stretched too far. Some brachial plexus injuries can occur in babies during birth.
What is the largest plexus in the body?
The solar plexus is the largest autonomic plexus and gives supply to multiple abdominal and pelvic organs. The superior mesenteric plexus comprises the superior mesenteric ganglia and is situated around the superior mesenteric artery.
Where do plexuses form?
There are two major nerve plexuses: the brachial plexus and the lumbosacral plexus. The brachial plexus come out from the cervical spine and the lumbosacral plexus come out from the lumbosacral spine.
What does the lumbar plexus give rise to?
The lumbar plexus originates from different branches which supply other muscles and regions of the posterior abdominal wall and lower limb. These branches comprise the iliohypogastric, ilioinguinal, genitofemoral, lateral femoral cutaneous, femoral, and obturator nerves.
What is the treatment for the lumbar plexus?
Treatment for Lumbosacral plexopathy depends upon the underlying causes. Symptomatic management with analgesics and muscle relaxants should be provided. Analgesics comprise non-steroidal anti-inflammatory drugs (NSAIDs), gabapentin, pregabalin, amitriptyline, duloxetine, and opioids.
What is the lumbar plexus made of?
The lumbar plexus is a web of nerves (a nervous plexus) in the lumbar area of the body which forms a portion of the larger lumbosacral plexus. It is formed by the divisions of the first four lumbar nerves (L1-L4) and from the offering of the subcostal nerve (T12), which is the last thoracic nerve.
Where does the lumbar plexus arise from?
The lumbosacral plexus is comprised of the anterior rami (i.e., branches) of spinal nerves L4 to L5 and S1 to S4. It is situated on the posterolateral wall of the lesser pelvis, near the lumbar spine. The lumbosacral plexus then inserts itself into the psoas major muscle and later comes out in the pelvis.
How many divisions do the lumbar plexus have?
The lumbar plexus is comprised of anterior and posterior divisions. The anterior division gives origin to the ilioinguinal, iliohypogastric, and genitofemoral nerves, all of which are obtained from L1–L2 and give sensory supply to the lower abdomen, upper proximal thigh, and lateral genitalia.
What causes lumbar plexus injury?
causes
Direct trauma. Posterior hip dislocation.
Radiation therapy or treatment of abdominal and pelvic malignancies (cancer).
Pregnancy-related.
Infections and local abscesses.
Postoperative plexopathy.
injury to the vessels supplies the Lumbosacral plexus.
Metabolic, inflammatory, and autoimmune causes:




7 Comments