
Trapezius Muscle
Introduction
The trapezius muscle is a large, superficial muscle located in the upper back and neck region of the human body. It is one of the major muscles responsible for the movement and stability of the shoulder girdle. Its name originates from its trapezoid shape, with its broad base spanning the upper back and its narrow apex extending towards the neck.
The trapezius is a large paired surface muscle that extends longitudinally from the occipital bone to the lower thoracic vertebrae of the spine and laterally to the spine of the scapula.
It moves the scapula and supports the arm.
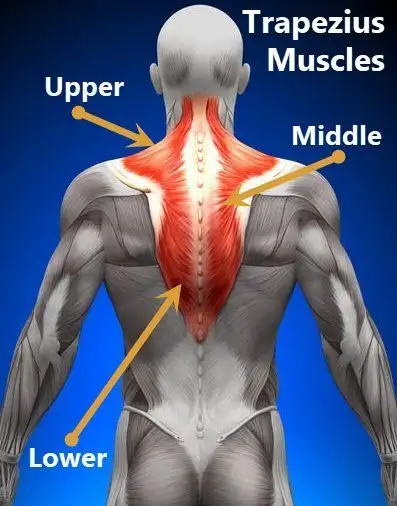
The trapezius has three functional parts:
- An upper (descending) part that supports the weight of the arm.
- A middle region (transverse), which retracts the scapula.
- A lower (ascending) part medially rotates and depresses the scapula.
Anatomy of Trapezius Muscle
As mentioned above, the trapezius muscle is divided into 3 areas: The upper fibers, the middle fibers (called the middle trapezius), and the lower fibers (called the lower traps).
The division into the separate, distinct parts of this muscle is about functionality. In other words, each area does something different.
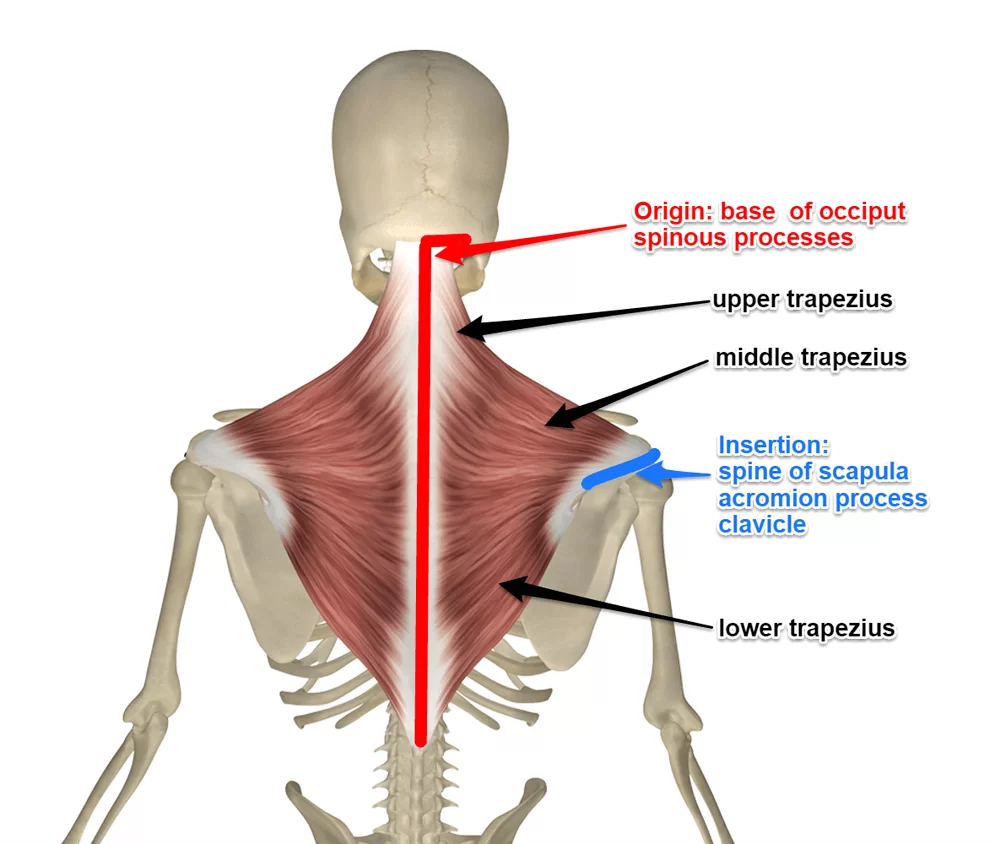
The upper trapezius arises from your occipital bone in the back of your skull and the nuchal line in the back of your neck.
The muscle also has attachments to the spinous processes of cervical levels one through six via the ligamentum nuchae.
Attachments of the lower fibers of the trapezius arise from the spinous processes of cervical seven through thoracic level 12.
The muscular fibers of the triangular-shaped traps travel to insert on the spine of the scapula and the acromion of the scapula.
They also attach to the outer one-third of the clavicle or collarbone.
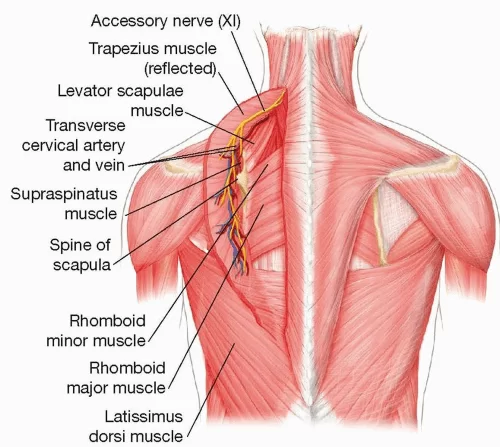
The trapezius belongs to the superficial layer of the extrinsic muscles of the back, along with latissimus dorsi, rhomboid major and minor, and levator scapulae muscles.
The trapezius is largely involved in movements of the shoulder girdle and is therefore functionally considered as a muscle of the upper limb rather than of the back.
Origin and Insertion of Trapezius Muscle
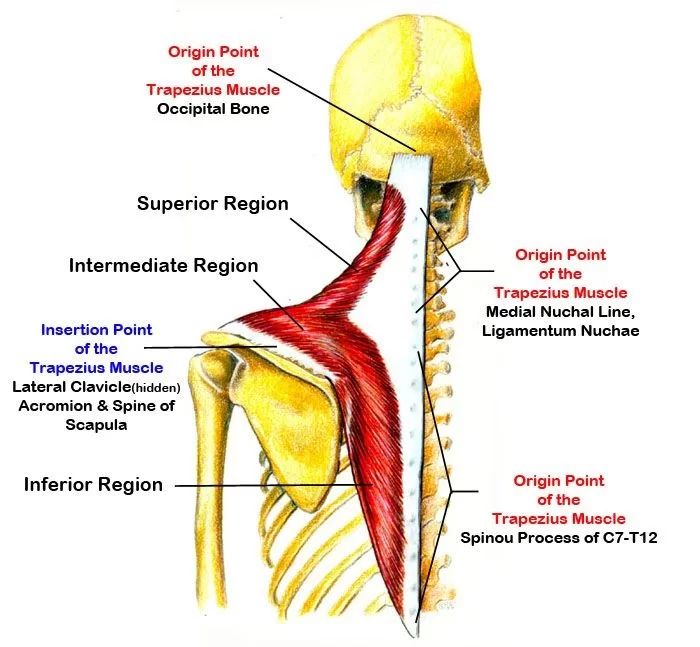
Superior nuchal line of occipital bone (Linea nuchalis superior ossis occipitalis).
The trapezius muscle has several origin points along the midline of the posterior neck and back.
The superior fibers attach on the medial third of the superior nuchal line and the external occipital protuberance of the occipital bone.
These fibers have a descending course towards their insertion point, hence why this part of the trapezius is referred to as the descending part.
The middle fibers originate from the nuchal ligament, that is attached to the spinous processes of the C1-C6 vertebrae, as well as the spinous processes of C7-T3 vertebrae and their intervening supraspinous ligaments.
These fibers are directed horizontally, running laterally towards the shoulder. Thus, these fibers represent the transverse part of the trapezius.
The inferior fibers originate from the spinous processes of the T4-T12 vertebrae and their respective supraspinous ligaments.
These fibers course superiorly and laterally towards their insertion point and hence, represent the ascending part of the trapezius.
Spine of scapula (Spina scapulae):
- Along their course, all fibers of the trapezius converge laterally on the superior angle of the scapula to attach on their respective insertion points.
- The superior fibers insert on the posterior border of the lateral third of the clavicle.
- The middle fibers insert onto the medial margin of the acromion of the scapula, as well as the superior crest of the scapular spine.
- The inferior fibers insert via aponeurosis on a tubercule at the lateral apex of the medial end of the scapular spine.
Structure
The trapezius muscle resembles a trapezium (trapezoid in American English), or diamond-shaped quadrilateral.
The word “spinotrapezius” refers to the human trapezius, although it is not commonly used in modern texts.
In other mammals, it refers to a portion of the analogous muscle.
The term “tri-axle back plate” was historically used to describe the trapezius muscle.
Position of the trapezius and its parts.
- Superior fibers of the trapezius
- Middle fibers of the trapezius
- Inferior fibers of the trapezius
The superior or upper (or descending) fibers of the trapezius originate from the spinous process of C7, the external occipital protuberance, the medial third of the superior nuchal line of the occipital bone (both in the back of the head), and the ligamentum nuchae.
From this origin they proceed downward and laterally to be inserted into the posterior border of the lateral third of the clavicle.
The middle fibers, or transverse of the trapezius arise from the spinous process of the seventh cervical (both in the back of the neck), and the spinous processes of the first, second, and third thoracic vertebrae.
They are inserted into the medial margin of the acromion, and into the superior lip of the posterior border of the spine of the scapula.
The inferior or lower (or ascending) fibers of the trapezius arise from the spinous processes of the remaining thoracic vertebrae (T4–T12).
From this origin they proceed upward and laterally to converge near the scapula and end in an aponeurosis, which glides over the smooth triangular surface on the medial end of the spine, to be inserted into a tubercle at the apex of this smooth triangular surface.
At its occipital origin, the trapezius is connected to the bone by a thin fibrous lamina, firmly adherent to the skin.
The superficial and deep epimysia are continuous with an investing deep fascia that encircles the neck and also contains both sternocleidomastoid muscles.
In the middle, the muscle is connected to the spinous processes by a broad semi-elliptical aponeurosis, which reaches from the sixth cervical to the third thoracic vertebrae and forms, with that of the opposite muscle, a tendinous ellipse.
The rest of the muscle arises by numerous short tendinous fibers.
It is possible to feel the muscles of the superior trapezius become active by holding a weight in one hand in front of the body and, with the other hand, touching the area between the shoulder and the neck.
Nerve Supply
- Spinal root of accessory nerve (CN XI) (motor).
- Cervical nerves (C3 and C4) (pain and proprioception).
- The trapezius muscle is the only muscle of the upper limb that does not receive its innervation from the brachial plexus.
- Motor innervation to the trapezius is conveyed by the accessory nerve (CN XI), while sensory innervation stems from the ventral rami of the C3 and C4 spinal nerves.
Blood Supply
- Occipital artery (Arteria occipitalis)
- The arterial supply to the trapezius varies depending on the level.
- The descending (upper) part of the muscle is supplied by transverse muscular branches arising from the occipital artery (branch of the external carotid), which passes along the deep surface of the muscle.
- The transverse (middle) part of the muscle is supplied by the superficial cervical artery, or by a branch from the transverse cervical artery.
- The ascending (lower) part is supplied by muscular branches of the dorsal scapular artery, which arises from the subclavian artery.
Function of Trapezius Muscle
The main function of the trapezius is stabilizing the scapula in its anatomical place, as well as controlling it during movements of the shoulder and upper limb.
The throwing action is a common maneuver in which the trapezius muscle is active, along with the deltoid muscle and the rotator cuff muscles.
The trapezius is also involved in the movements of the head and neck.
The actions of the trapezius muscle are largely dependent on the direction of the fibres that are contracting.
Descending (upper) fibers (Scapular movements)
Lateral flexion of the neck (Flexio lateralis cervicis)
Spinal movements: When the scapulae are stable a co-contraction of both sides can extend the neck.
- The descending (upper) fibers act with the levator scapulae muscle to produce an elevation of the scapula at the scapulothoracic joint.
- In the same manner, they also maintain the level of the shoulders against gravity e.g. when a weight is being carried in the hand.
- When the muscle is acting unilaterally, the descending fibres produce an ipsilateral lateral flexion of the head and neck by acting on the atlanto-occipital joint and upper cervical vertebrae, respectively.
- Unilateral contraction may also result in contralateral rotation of the head at the atlantoaxial joint.
- Bilateral contraction of the descending part of the trapezius (i.e. when both left and right muscles contract) causes an extension of the head and neck.
Ascending (lower) fibers:
- The ascending (lower) fibers are responsible for the depression of the medial part of the scapula, and thus lowering the shoulder.
- This action is especially important for activities in which the shoulders are lowered against resistance, for example when using the hands to help oneself up from a seated position.
- Together with the descending part, the ascending fibers also produce a rotation of the scapula around an axis that runs anteroposteriorly through the base of the scapular spine.
Transverse (middle) fibers:
- The transverse (middle) fibers act together with the rhomboids to produce a retraction of the scapula, by pulling it towards the midline.
- The trapezius muscle is also responsible for the upward rotation of the scapula, along with the serratus anterior muscle.
- This allows us to raise our arms above our heads beyond the level of the shoulder.
Action
Descending part: Elevates pectoral girdle
Middle part: Retracts scapula
Ascending part: Depresses shoulders
Descending and ascending together: Rotates scapula upwards
Bilateral contraction: Extends neck
Unilateral contraction: Ipsilateral side flexion of the neck
Middle part: Assists with ipsilateral side flexion and contralateral axial rotation of the upper thoracic region.
Relation
The trapezius is the most superficial of the superficial extrinsic back muscles, together with the latissimus dorsi. It rests on top of the other muscles in this group, which include the levator scapulae and rhomboids.
The serratus posterior superior, a member of the intermediate layer of the back’s extrinsic muscles, is located deep within the trapezius muscle.
Additionally, the splenius capitis, splenius cervicis, spinalis, longissimus, and iliocostalis muscles comprise the muscles of the superficial layer of the intrinsic muscle group that has been covered by the trapezius. The suboccipital region is likewise served by the upper portion of the trapezius.
Anatomical Variations
Although statistically rare, anatomic variations of the trapezius muscle are significant and variable. Many of those variations are embryonic in nature and are associated with unilateral or bilateral development of the trapezius, which causes hypoplasia or the development of auxiliary muscle lobes.
In one reported case of heritable missing of the trapezius muscle, the absence of the muscle was also seen in the daughter of two parents who lacked the muscle.
Other defects consist of hypoplasia of the trapezius muscles caused by the dysfunction or absence of the spinal auxiliary nerve (CN XI), not their real disappearance.
Clinical Importance
Dysfunction of the trapezius result can result in a winged scapula, sometimes further specified as “lateral winging” and in abnormal mobility or function of the scapula (scapular dyskinesia).
There are multiple causes of trapezius dysfunction.
Palsy:
- Trapezius palsy, due to damage of the spinal accessory nerve, is characterized by difficulty with arm adduction and abduction, and associated with a drooping shoulder, and shoulder and neck pain.
- Intractable trapezius palsy can be surgically managed with an Eden-Lange procedure.
Facioscapulohumeral muscular dystrophy:
- The trapezius muscle is one of the commonly affected muscles in facioscapulohumeral muscular dystrophy (FSHD).
- The lower and middle fibers are affected initially, and the upper fibers are commonly spared until late in the disease.
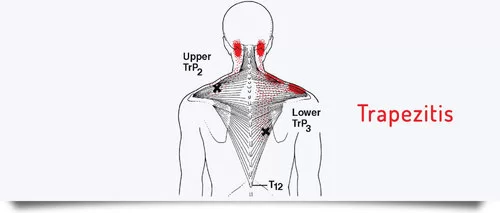
Trigger Point Referral Pattern:
Techniques:
Palpation
- Superficial, can palpate upper, middle, and lower
- Upper is frequently involved in neck injuries
- Hold the sloping superior lateral portion between fingers and thumb and palpate from
- origin (O) toward the clavicle/acromion and its insertion (I)
With patient (pt.) standing: Abduct shoulders to 90 degrees and retract shoulder girdle.
Slightly bend the trunk forward so antigravity.
Upper can also be seen with elevation and lower with depression.
Length Tension Testing:
- Patient: Positioned in supine lying with the arms resting by the side and the knees flexed.
- Therapist: Standing at the head of the bed.
- Action: The therapist supports the posterior aspect of the head with both hands and then passively flexes the craniovertebral joint.
The right hand stabilizes the lateral one-third of the patient’s right clavicle and acromion palpating the muscle.
The therapist then gently and slowly flexes, the left side flexes and the right rotates the mid and lower cervical spine with the left hand.
The hand stabilizing and the hand moving the body part senses the tension in the muscle and barrier.
The amount of range and the end feel is assessed and the reproduction of any symptoms is noted.
This test is then repeated on the contralateral side and compared.
TRAPEZIUS MUSCLE PAIN TREATMENT
Trapezius muscle pain is a most common condition mainly due to overuse of the muscle during day-to-day activities. Pain and muscle spasm mainly in the upper trapezius is more common in females.
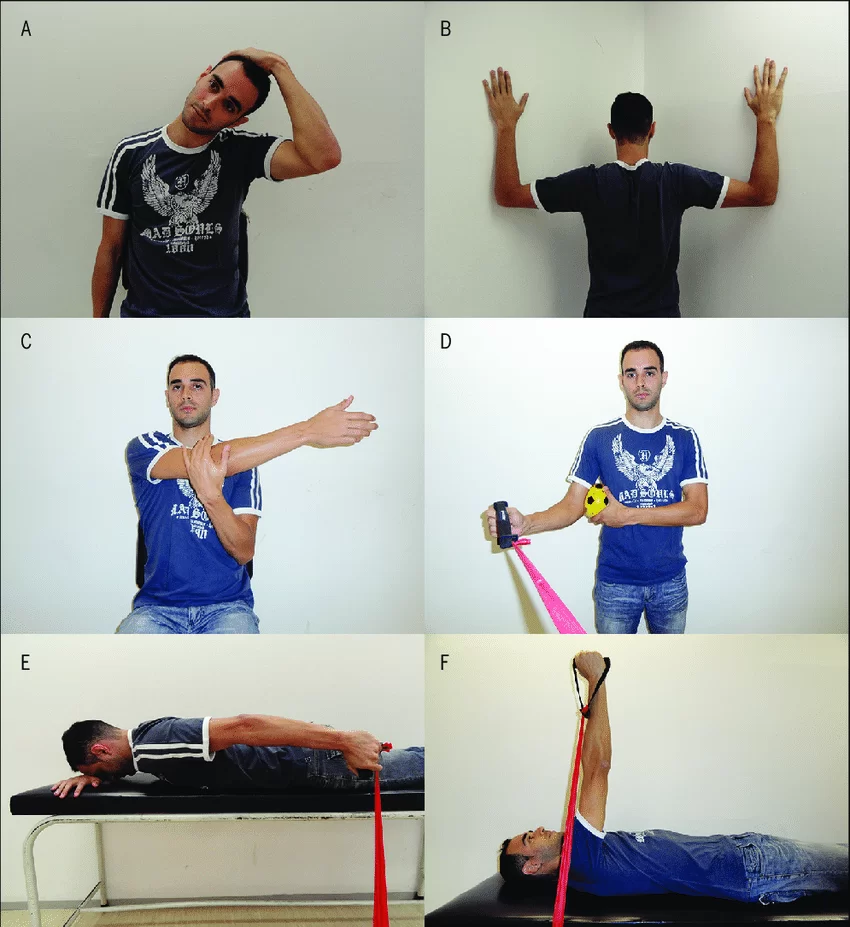
EXERCISE:
- Tight upper trapezius muscles often respond well to massage therapy. And because they are located such that you can reach your own, you might consider trying a self-massage technique.
- A massage therapist skilled in the art of myofascial release may be able to help you though.
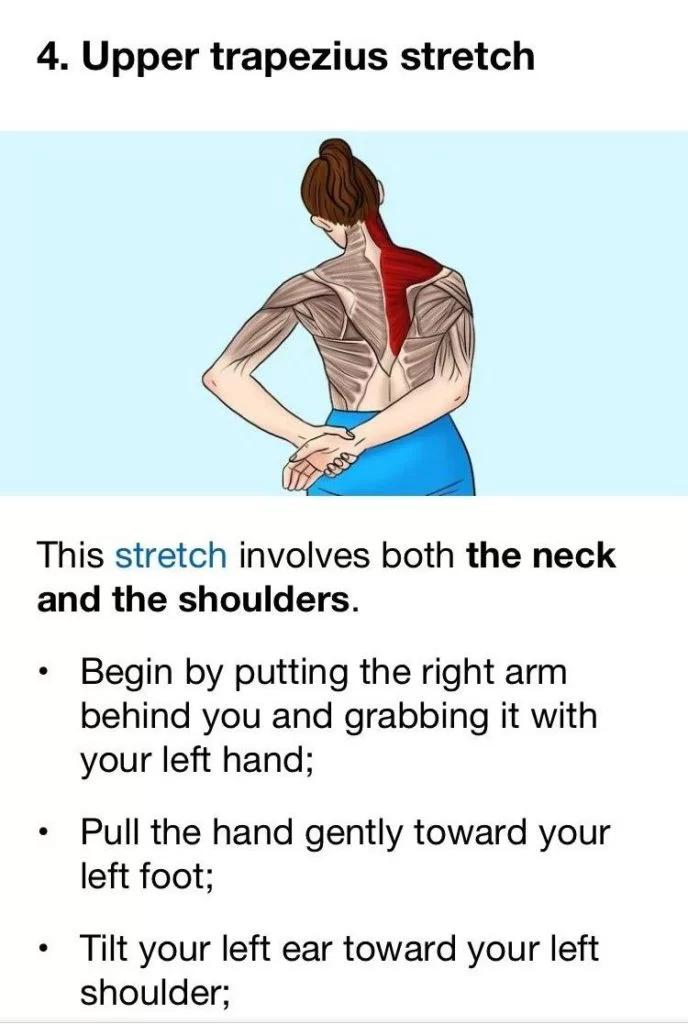
Stretching:
- Sit upright in a chair and make sure that your posture is correct.
- These stretches can be done in repetitions of 15-20 every hour to decrease trapezius muscle pain.
- Begin by rolling the shoulders back so that the shoulder blades feel like they are being pinched together.
- Then raise your shoulders up towards the ceiling and lower them down gently.
- You can then bend your neck from side to side by tilting your head towards your shoulder and counting to 3, then repeating in each direction.
Massage:
- Pain in the shoulder and neck can be prevented or reduced with massage.
- It is possible to reduce trapezius muscle pain through self-massage. Reach back with one hand and find your trapezius muscle.
- Beginning at the base of the neck, try to knead the trapezius muscles.
Pressure:
- Some pressure can also apply to the area along your shoulders and between the shoulder blades.
- If there is an area that is more tender, apply pressure for ten seconds and then release it so that the muscle can relax.
Summary
Overall, the trapezius muscle’s complex anatomy and function make it an essential component of the musculoskeletal system, contributing significantly to the stability and mobility of the upper back and neck.
FAQs
What causes trapezius muscle pain?
The trapezius muscle is susceptible to tension and pain due to factors like poor posture, repetitive movements, and stress. Conditions such as trapezius muscle strain, trigger points, and myofascial pain syndrome can result in discomfort and restricted shoulder and neck movement. Proper stretching, strengthening exercises, and postural awareness can aid in the prevention and management of such issues.
How do you fix trapezius pain?
The following tips is the best options to fix trapezius pain:
Rest and avoid aggravating painful activities
Apply heat or cold packs
Gentle Stretching exercises
Gradual Strengthening exercises
Posture awareness
Massage and self-myofascial release
Pain relief medications
Avoid heavy bags or backpacks
Stress management
Physical therapy
Why are my trap muscles so big?
Long-term strain on the trapezius muscle causes it to grow bigger and stronger, which results in a thicker shoulder. In addition to improper postures, our breathing patterns, movement patterns, and walking patterns can all influence how well the trapezius muscles are used.
Is trapezius pain permanent?
Trapezius pain is not necessarily permanent, and in many cases, it can be managed and relieved with appropriate treatments and self-care. However, the duration and outcome of trapezius pain depend on several factors, including the underlying cause, the severity of the condition, and how well it is managed.
Does massage help trapezius pain?
Massage treatment relaxes tense muscles and increases blood flow to relieve inflammation by applying pressure to specific regions. Trapezius strain pain has been demonstrated to decrease with massage, and the affected areas’ mobility has also been shown to improve.
Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803


33 Comments